

Clinical presentation, etiology, and survival in adult acute encephalitis syndrome in rural Central India
- PMID: 23643180
- PMCID: PMC3786210
- DOI: 10.1016/j.clineuro.2013.04.008
Clinical presentation, etiology, and survival in adult acute encephalitis syndrome in rural Central India
Abstract
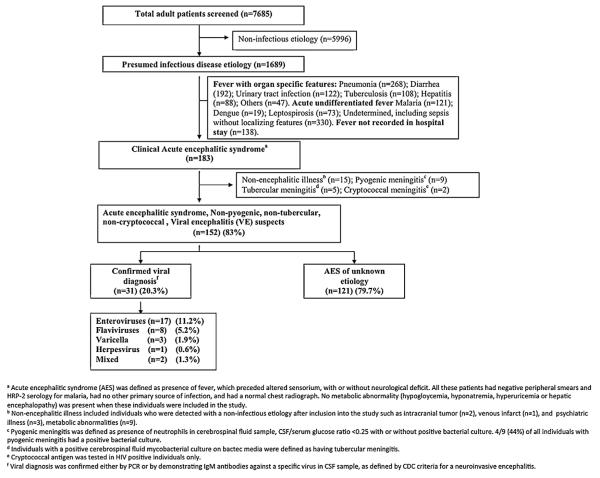
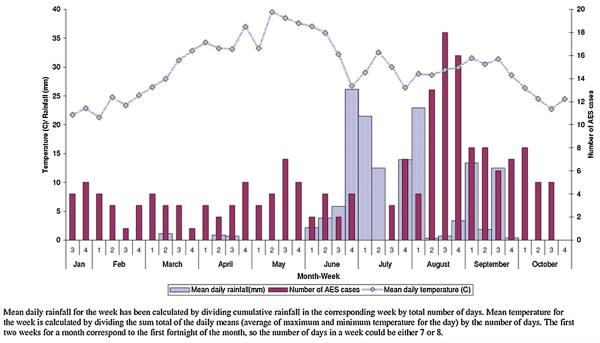
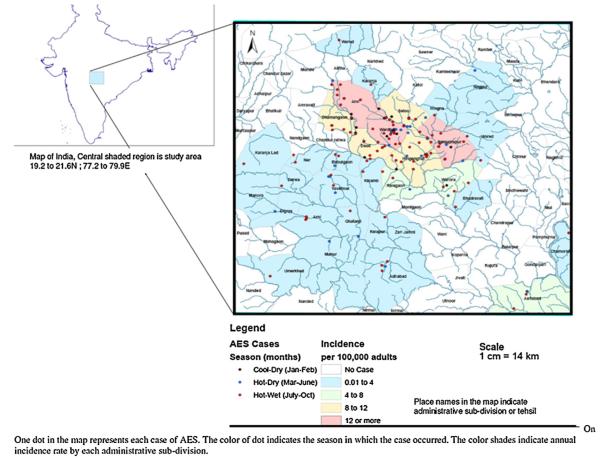
Background: Acute encephalitis syndrome (AES) is a constellation of symptoms that includes fever and altered mental status. Most cases are attributed to viral encephalitis (VE), occurring either in outbreaks or sporadically. We conducted hospital-based surveillance for sporadic adult-AES in rural Central India in order to describe its incidence, spatial and temporal distribution, clinical profile, etiology and predictors of mortality.
Methods: All consecutive hospital admissions during the study period were screened to identify adult-AES cases and were followed until 30-days of hospitalization. We estimated incidence by administrative sub-division of residence and described the temporal distribution of cases. We performed viral diagnostic studies on cerebrospinal fluid (CSF) samples to determine the etiology of AES. The diagnostic tests included RT-PCR (for enteroviruses, HSV 1 and 2), conventional PCR (for flaviviruses), CSF IgM capture ELISA (for Japanese encephalitis virus, dengue, West Nile virus, Varicella zoster virus, measles, and mumps). We compared demographic and clinical variables across etiologic subtypes and estimated predictors of 30-day mortality.
Results: A total of 183 AES cases were identified between January and October 2007, representing 2.38% of all admissions. The incidence of adult AES in the administrative subdivisions closest to the hospital was 16 per 100,000. Of the 183 cases, a non-viral etiology was confirmed in 31 (16.9%) and the remaining 152 were considered as VE suspects. Of the VE suspects, we could confirm a viral etiology in 31 cases: 17 (11.2%) enterovirus; 8 (5.2%) flavivirus; 3 (1.9%) Varicella zoster; 1 (0.6%) herpesvirus; and 2 (1.3%) mixed etiology); the etiology remained unknown in remaining 121 (79.6%) cases. 53 (36%) of the AES patients died; the case fatality proportion was similar in patients with a confirmed and unknown viral etiology (45.1 and 33.6% respectively). A requirement for assisted ventilation significantly increased mortality (HR 2.14 (95% CI 1.0-4.77)), while a high Glasgow coma score (HR 0.76 (95% CI 0.69-0.83)), and longer duration of hospitalization (HR 0.88 (95% CI 0.83-0.94)) were protective.
Conclusion: This study is the first description of the etiology of adult-AES in India, and provides a framework for future surveillance programs in India.
Keywords: Acute encephalitis syndrome; Adults; Central India; Rural; Viral encephalitis.
Copyright © 2013 Elsevier B.V. All rights reserved.
Figures

References
-
- Mathur A, Chaturvedi UC, Tandon HO, Agarwal AK, Mathur GP, Nag D, et al. Japanese encephalitis epidemic in Uttar Pradesh, India during 1978. Indian Journal of Medical Research. 1982;75:161–9. - PubMed
-
- Vajpayee A, Dey PN, Chakraborty AK, Chakraborty MS. Study of the outbreak of Japanese encephalitis in Lakhimpur district of Assam in 1989. Journal of the Indian Medical Association. 1992;90:114–5. - PubMed
-
- Kar NJ, Saxena VK. Some epidemiological characteristics of Japanese encephalitis in Haryana state of northern India. Journal of Communicable Diseases. 1998;30:129–31. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
