

Low to moderate dose anthracycline-based chemotherapy is associated with early noninvasive imaging evidence of subclinical cardiovascular disease
- PMID: 23643285
- PMCID: PMC3745801
- DOI: 10.1016/j.jcmg.2012.11.017
Low to moderate dose anthracycline-based chemotherapy is associated with early noninvasive imaging evidence of subclinical cardiovascular disease
Abstract
Objectives: The goal of this study was to determine if low to moderate doses of anthracycline-based chemotherapy (Anth-bC) are associated with subclinical cardiovascular (CV) injury.
Background: Cancer survivors who receive Anth-bC experience premature CV events. It is unknown whether low to moderate doses of anthracyclines promote early subclinical CV disease manifested by deteriorations in left ventricular ejection fraction (LVEF) or increases in aortic stiffness, or if these doses are associated with changes in quality of life (QOL).
Methods: In 53 men and women with breast cancer, leukemia, or lymphoma, we assessed left ventricular volumes, LVEF, circumferential strain, aortic pulse wave velocity, late gadolinium enhancement, serum B-type natriuretic peptide, troponin I, and the impact of treatment on QOL before and 1, 3, and 6 months after receipt of Anth-bC.
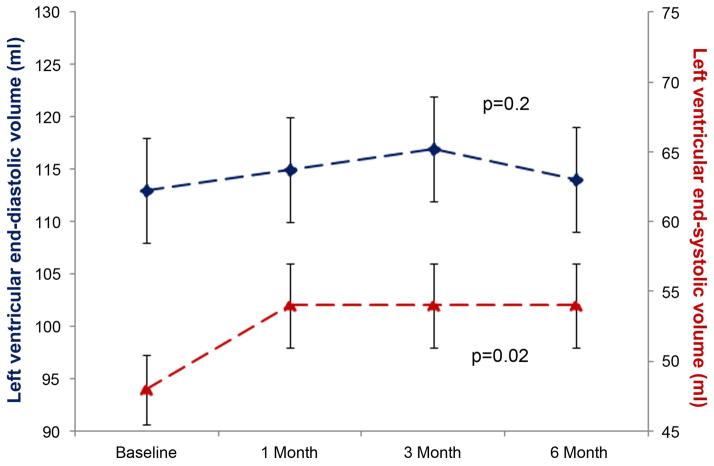
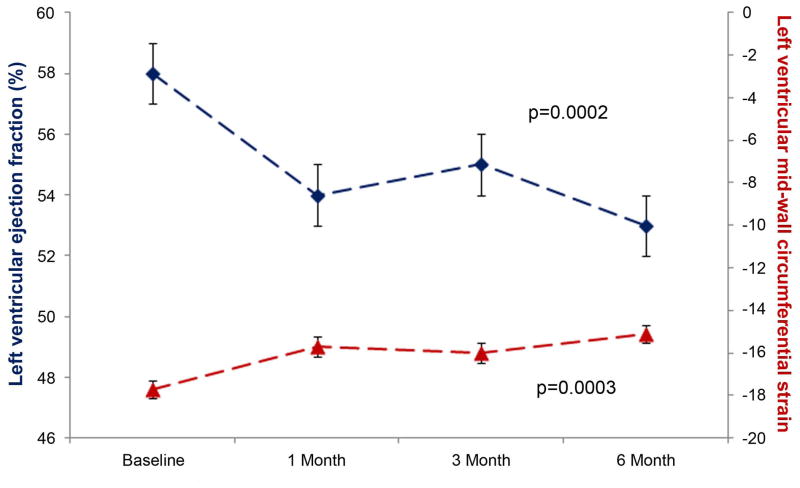
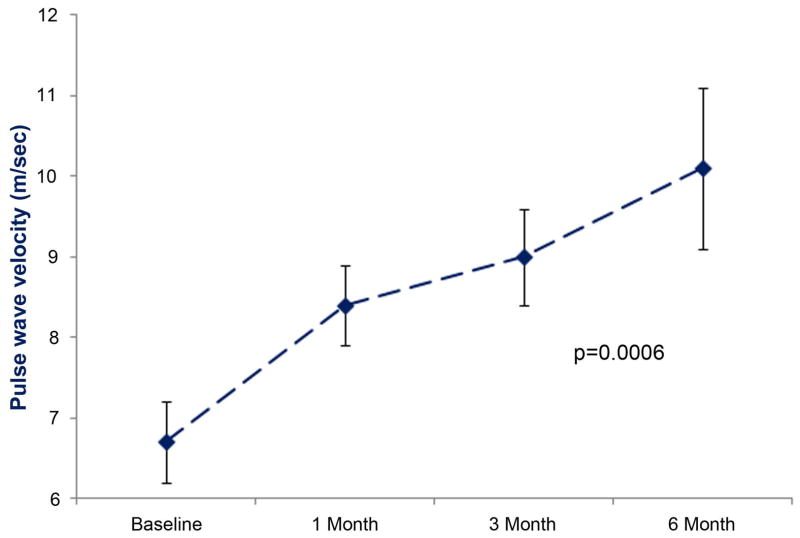
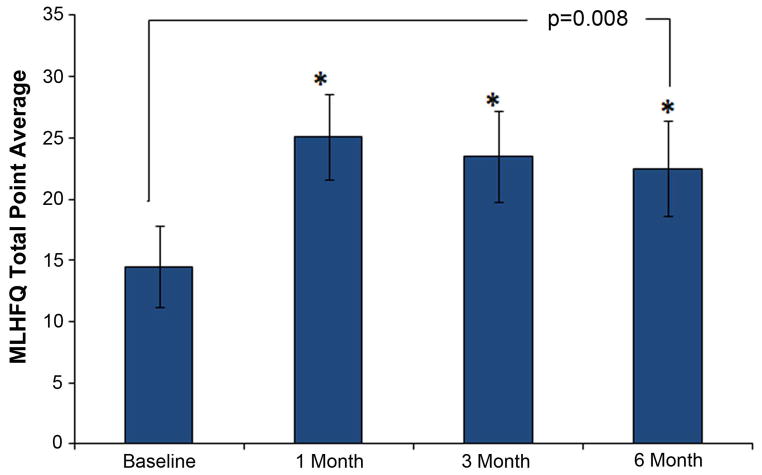
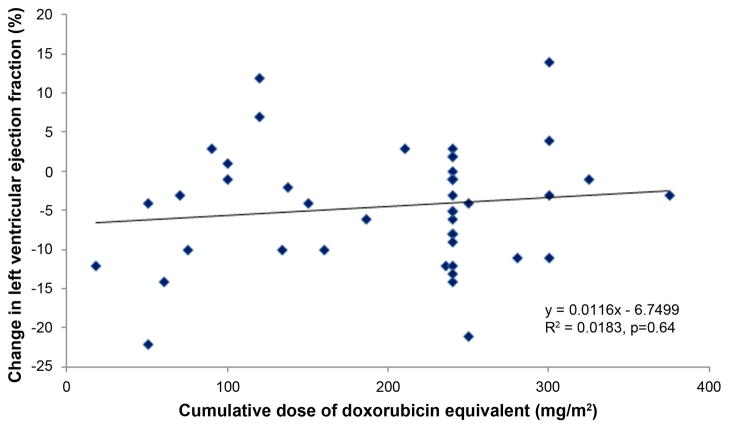
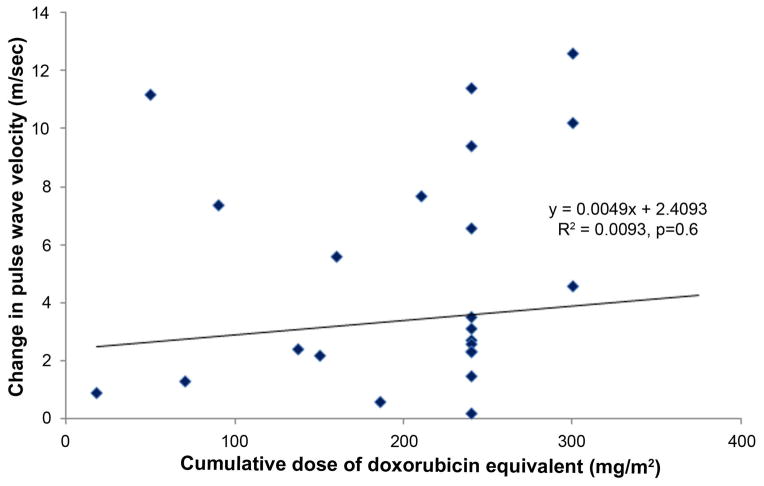
Results: Participants averaged 50 ± 2 (range 19 to 80) years in age, 58% were women, 17% were black, and they each received a range of 50 to 375 mg/m(2) of doxorubicin-equivalent chemotherapy. Left ventricular end-systolic volume (48 ± 3 ml to 54 ± 3 ml; p = 0.02), left ventricular strain (-17.7 ± 0.4 to -15.1 ± 0.4; p = 0.0003), pulse wave velocity (6.7 ± 0.5 m/s to 10.1 ± 1 m/s; p = 0.0006), and QOL deterioration (15.4 ± 3.3 to 28.5 ± 3.9; p = 0.008) increased, whereas LVEF (58 ± 1% to 53 ± 1%; p = 0.0002) decreased within 6 months after low to moderate doses of Anth-bC. All findings persisted after accounting for age, gender, race (white/black), doxorubicin-equivalent dose, doxorubicin administration technique, comorbidities associated with CV events, and cancer diagnosis (p = 0.02 to 0.0001 for all). There were no new late gadolinium enhancement findings after 6 months.
Conclusions: In these study patients, low to moderate doses of Anth-bC were associated with the early development of subclinical abnormalities of cardiac and vascular function that in other populations are associated with the future occurrence of CV events.
Keywords: Anth-bC; B-type natriuretic peptide; BNP; CMR; CV; LVEDV; LVEF; LVESV; MLHFQ; Minnesota Living with Heart Failure Questionnaire; PWV; QOL; TE; TR; TnI; anthracycline-based chemotherapy; cardiac magnetic resonance; cardio-oncology; cardiotoxicity; cardiovascular; chemotherapy; echo time; left ventricular ejection fraction; left ventricular end-diastolic volume; left ventricular end-systolic volume; pulse wave velocity; quality of life; repetition time; troponin I.
Copyright © 2013 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
The red devil revisited.JACC Cardiovasc Imaging. 2013 Aug;6(8):886-8. doi: 10.1016/j.jcmg.2013.04.009. JACC Cardiovasc Imaging. 2013. PMID: 23948379 No abstract available.
References
-
- Hooning MJ, Botma A, Aleman BM, et al. Long-term risk of cardiovascular disease in 10-year survivors of breast cancer. J Natl Cancer Inst. 2007;99:365–75. - PubMed
-
- Swerdlow AJ, Higgins CD, Smith P, et al. Myocardial infarction mortality risk after treatment for Hodgkin’s disease: A collaborative British cohort study. J Natl Cancer Inst. 2007;99:206–14. - PubMed
-
- Singal PK, Iliskovic N. Doxorubicin-induced cardiomyopathy. N Eng J Med. 1998;339:900–5. - PubMed
-
- Eschenhagen T, Force T, Ewer MS, et al. Cardiovascular side effects of cancer therapies: a position statement from the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2011;13:1–10. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
