

Defining sedation-related adverse events in the pediatric intensive care unit
- PMID: 23643411
- PMCID: PMC3641854
- DOI: 10.1016/j.hrtlng.2013.02.004
Defining sedation-related adverse events in the pediatric intensive care unit
Abstract
Background: Clinical trials exploring optimal sedation management in critically ill pediatric patients are urgently needed to improve both short- and long-term outcomes. Concise operational definitions that define and provide best-available estimates of sedation-related adverse events (AE) in the pediatric population are fundamental to this line of inquiry.
Objectives: To perform a multiphase systematic review of the literature to identify, define, and provide estimates of sedation-related AEs in the pediatric ICU setting for use in a multicenter clinical trial.
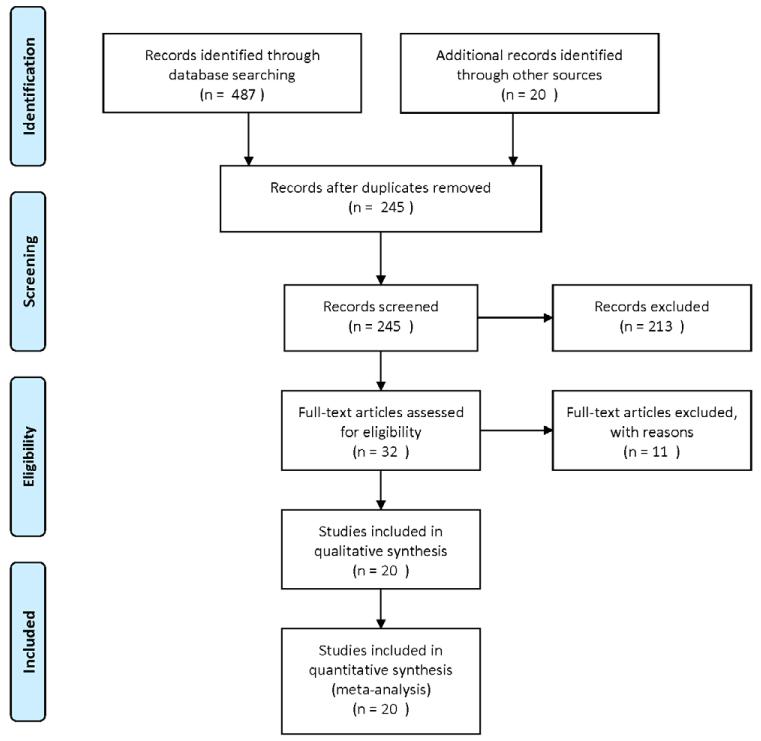
Methods: In Phase One, we identified and operationally defined the AE. OVID-MEDLINE and CINAHL databases were searched from January 1998 to January 2012. Key terms included sedation, intensive and critical care. We limited our search to data-based clinical trials from neonatal to adult age. In Phase Two, we replicated the search strategy for all AEs and identified pediatric-specific AE rates.
Results: We reviewed 20 articles identifying sedation-related adverse events and 64 articles on the pediatric-specific sedation-related AE. A total of eleven sedation-related AEs were identified, operationally defined and estimated pediatric event rates were derived. AEs included: inadequate sedation management, inadequate pain management, clinically significant iatrogenic withdrawal, unplanned endotracheal tube extubation, post-extubation stridor with chest-wall retractions at rest, extubation failure, unplanned removal of invasive tubes, ventilator-associated pneumonia, catheter-associated bloodstream infection, Stage II+ pressure ulcers and new tracheostomy.
Conclusions: Concise operational definitions that defined and provided best-available event rates of sedation-related AEs in the pediatric population are presented. Uniform reporting of adverse events will improve subject and patient safety.
Copyright © 2013 Elsevier Inc. All rights reserved.
References
-
- Rhoney DH, Murry KR. National survey on the use of sedatives and neuromuscular blocking agents in the pediatric intensive care unit. Pediatr Crit Care Med. 2002;3:129–133. - PubMed
-
- Twite MD, Rashid A, Zuk J, et al. Sedation, analgesia, and neuromuscular blockade in the pediatric intensive care unit: survey of fellowship training programs. Pediatr Crit Care Med. 2004;5:521–532. - PubMed
-
- Marx CM, Rosenberg DI, Ambuel B, et al. Pediatric intensive care sedation: survey of fellowship training programs. Pediatrics. 1993;91:369–378. - PubMed
-
- Barrientos-Vega R, Mar Sanchez-Soria M, Morales-Garcia C, et al. Prolonged sedation of critically ill patients with midazolam or propofol: impact on weaning and costs. Crit Care Med. 1997;25:33–40. - PubMed
-
- Kress JP, Pohlman AS, Hall JB. Sedation and analgesia in the intensive care unit. Am J Respir Crit Care Med. 2002;166:1024–0128. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
