

The role of different anesthetic techniques in altering the stress response during cardiac surgery in children: a prospective, double-blinded, and randomized study
- PMID: 23644384
- PMCID: PMC3885862
- DOI: 10.1097/PCC.0b013e31828a742c
The role of different anesthetic techniques in altering the stress response during cardiac surgery in children: a prospective, double-blinded, and randomized study
Abstract
Objectives: Our goal was to evaluate the role of three anesthetic techniques in altering the stress response in children undergoing surgery for repair of congenital heart diseases utilizing cardiopulmonary bypass in the setting of fast tracking or early tracheal extubation. Furthermore, we wanted to evaluate the correlation between blunting the stress response and the perioperative clinical outcomes.
Design: Prospective, randomized, double-blinded study.
Setting: Single center from December 2008 to May of 2011.
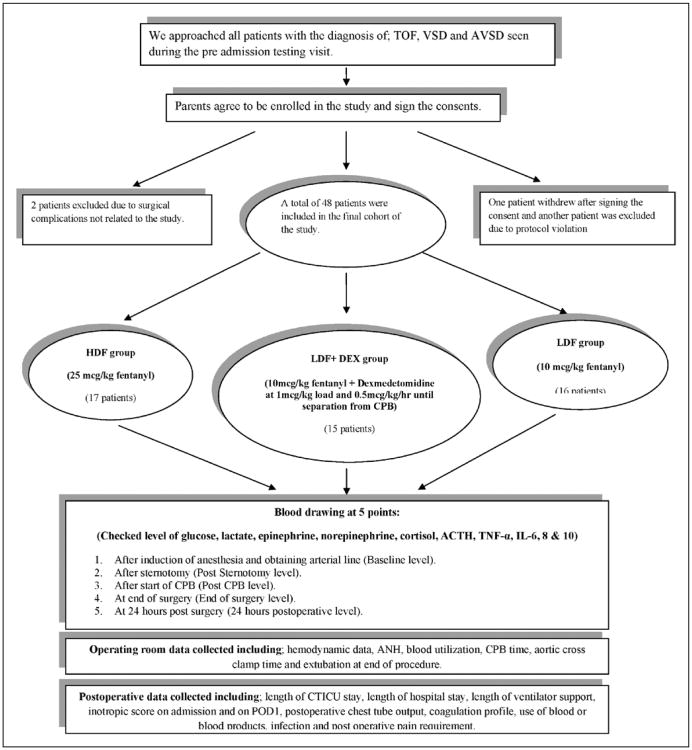
Patients: Forty-eight subjects (low-dose fentanyl plus placebo, n = 16; high-dose fentanyl plus placebo, n = 17; low-dose fentanyl plus dexmedetomidine, n = 15) were studied between ages 30 days to 3 years old who were scheduled to undergo repair for a ventricular septal defect, atrioventricular septal defect, or Tetralogy of Fallot.
Methods: Children undergoing surgical repair of congenital heart disease were randomized to receive low-dose fentanyl (10 mcg/kg; low-dose fentanyl), high-dose fentanyl (25mcg/kg; high-dose fentanyl), or low-dose fentanyl plus dexmedetomidine (as a 1 mcg/kg loading dose followed by infusion at 0.5mcg/kg/hr until separation from cardiopulmonary bypass. In addition, patients received a volatile anesthetic agent as needed to maintain hemodynamic stability. Blood samples were tested for metabolic, hormonal and cytokine markers at baseline, after sternotomy, after the start of cardiopulmonary bypass, at the end of the procedure and at 24 hours postoperatively.
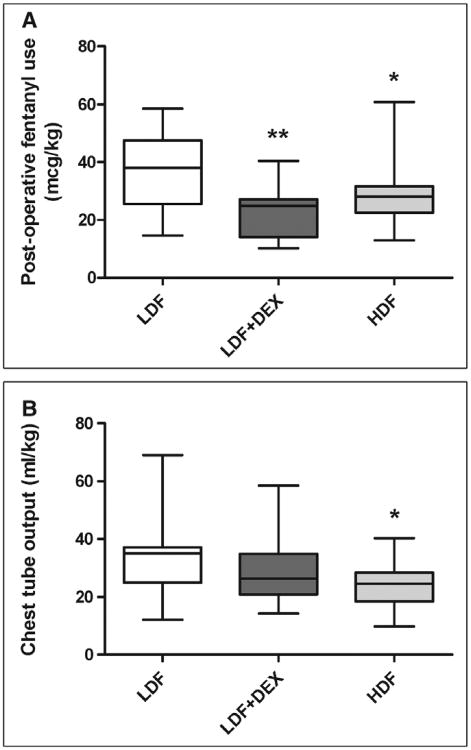
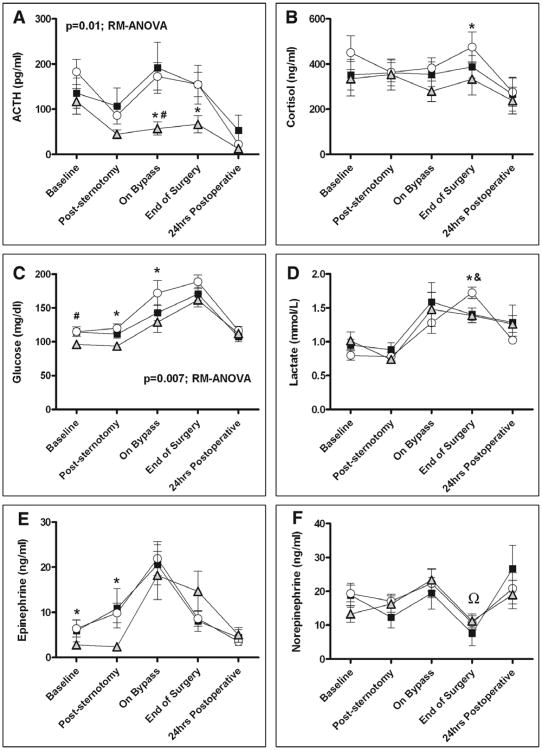
Measurements and main results: Forty-eight subjects (low-dose fentanyl plus placebo, n = 16; high-dose fentanyl plus placebo, n = 17; low-dose fentanyl plus dexmedetomidine, n = 15) were studied. Subjects in the low-dose fentanyl plus placebo group had significantly higher levels of adrenocorticotropic hormone, cortisol, glucose, lactate, and epinephrine during the study period. The lowest levels of stress markers were seen in the high-dose fentanyl plus placebo group both over time (adrenocorticotropic hormone, p= 0.01; glucose, p = 0.007) and at individual time points (cortisol and lactate at the end of surgery, epinephrine poststernotomy; p < 0.05). Subjects in the low-dose fentanyl plus dexmedetomidine group had lower lactate levels at the end of surgery compared with the low-dose fentanyl plus placebo group (p < 0.05). Although there were no statistically significant differences in plasma cytokine levels between the three groups, the low-dose fentanyl plus placebo group had significantly higher interleukin-6:interleukin-10 ratio at 24 hours postoperatively (p < 0.0001). In addition, when compared with the low-dose fentanyl plus placebo group, the low-dose fentanyl plus dexmedetomidine group showed a lower norepinephrine level from baseline at poststernotomy, after the start of cardiopulmonary bypass, and at the end of surgery (p ≤ 0.05). Subjects in the low-dose fentanyl plus placebo group had more postoperative narcotic requirement (p = 0.004), higher prothrombin time (p ≤ 0.03), and more postoperative chest tube output (p < 0.05). Success of fast tracking was not significantly different between groups (low-dose fentanyl plus placebo 75%, high-dose fentanyl plus placebo 82%, low-dose fentanyl plus dexmedetomidine 93%; p = 0.39).
Conclusions: The use of low-dose fentanyl was associated with the greatest stress response, most coagulopathy, and highest transfusion requirement among our cohorts. Higher dose fentanyl demonstrated more favorable blunting of the stress response. When compared with low-dose fentanyl alone, the addition of dexmedetomidine improved the blunting of the stress response, while achieving better postoperative pain control.
Figures
Comment in
-
Minimize stress and maximize clinical outcome!Pediatr Crit Care Med. 2013 Jun;14(5):547-8. doi: 10.1097/PCC.0b013e31828a8319. Pediatr Crit Care Med. 2013. PMID: 23867435 No abstract available.
Similar articles
-
Intrathecal versus IV fentanyl in pediatric cardiac anesthesia.Anesth Analg. 2002 Nov;95(5):1207-14, table of contents. doi: 10.1097/00000539-200211000-00017. Anesth Analg. 2002. PMID: 12401595 Clinical Trial.
-
Hemodynamic effects of the combination of dexmedetomidine-fentanyl versus midazolam-fentanyl in children undergoing cardiac surgery with cardiopulmonary bypass.Rev Bras Anestesiol. 2010 Jul-Aug;60(4):350-62. doi: 10.1016/S0034-7094(10)70044-1. Rev Bras Anestesiol. 2010. PMID: 20659607 Clinical Trial. English, Portuguese.
-
Stress response in infants undergoing cardiac surgery: a randomized study of fentanyl bolus, fentanyl infusion, and fentanyl-midazolam infusion.Anesth Analg. 2001 Apr;92(4):882-90. doi: 10.1097/00000539-200104000-00016. Anesth Analg. 2001. PMID: 11273919 Clinical Trial.
-
Effectiveness of dexmedetomidine versus propofol on extubation times, length of stay and mortality rates in adult cardiac surgery patients: a systematic review and meta-analysis.JBI Database System Rev Implement Rep. 2018 May;16(5):1220-1239. doi: 10.11124/JBISRIR-2017-003488. JBI Database System Rev Implement Rep. 2018. PMID: 29762314
-
Outcomes of dexmedetomidine treatment in pediatric patients undergoing congenital heart disease surgery: a meta-analysis.Paediatr Anaesth. 2016 Mar;26(3):239-48. doi: 10.1111/pan.12820. Epub 2015 Nov 27. Paediatr Anaesth. 2016. PMID: 26612740
Cited by
-
Anti-inflammatory Effects of Perioperative Dexmedetomidine Administered as an Adjunct to General Anesthesia: A Meta-analysis.Sci Rep. 2015 Jul 21;5:12342. doi: 10.1038/srep12342. Sci Rep. 2015. PMID: 26196332 Free PMC article.
-
One-year experience after adoption of an on-table extubation protocol following pediatric cardiac surgery.Ann Card Anaesth. 2022 Oct-Dec;25(4):422-428. doi: 10.4103/aca.aca_58_21. Ann Card Anaesth. 2022. PMID: 36254905 Free PMC article.
-
Changes in Anesthetic and Postoperative Sedation-Analgesia Practice Associated With Early Extubation Following Infant Cardiac Surgery: Experience From the Pediatric Heart Network Collaborative Learning Study.Pediatr Crit Care Med. 2019 Oct;20(10):931-939. doi: 10.1097/PCC.0000000000002005. Pediatr Crit Care Med. 2019. PMID: 31169762 Free PMC article.
-
A Review of the Biological Mechanisms of Dexmedetomidine for Postoperative Neurocognitive Disorders.Med Sci Monit. 2022 Oct 25;28:e937862. doi: 10.12659/MSM.937862. Med Sci Monit. 2022. PMID: 36281208 Free PMC article. Review.
-
The effect of modified ultrafiltration on angiopoietins in pediatric cardiothoracic operations.Ann Thorac Surg. 2014 Nov;98(5):1699-704. doi: 10.1016/j.athoracsur.2014.06.053. Epub 2014 Sep 23. Ann Thorac Surg. 2014. PMID: 25258157 Free PMC article.
References
-
- Anand KJ, Sippell WG, Aynsley-Green A. Randomised trial of fentanyl anaesthesia in preterm babies undergoing surgery: Effects on the stress response. Lancet. 1987;1:243–248. - PubMed
-
- Gajarski RJ, Stefanelli CB, Graziano JN, et al. Adrenocortical response in infants undergoing cardiac surgery with cardiopulmonary bypass and circulatory arrest. Pediatr Crit Care Med. 2010;11:44–51. - PubMed
-
- Gruber EM, Laussen PC, Casta A, et al. Stress response in infants undergoing cardiac surgery: A randomized study of fentanyl bolus, fentanyl infusion, and fentanyl-midazolam infusion. Anesth Analg. 2001;92:882–890. - PubMed
-
- Roth-Isigkeit A, Brechmann J, Dibbelt L, et al. Persistent endocrine stress response in patients undergoing cardiac surgery. J Endocrinol Invest. 1998;21:12–19. - PubMed
-
- Anand BK, Raghunath P, Dua S, et al. Hypothalamic control of the pituitary adrenocortical response to stress stimuli. Indian J Med Res. 1954;42:231–248. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
