

Clinical relevance and practical implications of trials of perfusion and angiographic imaging in patients with acute ischaemic stroke: a multicentre cohort imaging study
- PMID: 23644501
- PMCID: PMC3756443
- DOI: 10.1136/jnnp-2012-304807
Clinical relevance and practical implications of trials of perfusion and angiographic imaging in patients with acute ischaemic stroke: a multicentre cohort imaging study
Abstract
Background: In randomised trials testing treatments for acute ischaemic stroke, imaging markers of tissue reperfusion and arterial recanalisation may provide early response indicators.
Objective: To determine the predictive value of structural, perfusion and angiographic imaging for early and late clinical outcomes and assess practicalities in three comprehensive stroke centres.
Methods: We recruited patients with potentially disabling stroke in three stroke centres, performed magnetic resonance (MR) or CT, including perfusion and angiography imaging, within 6 h, at 72 h and 1 month after stroke. We assessed the National Institutes of Health Stroke Scale (NIHSS) score serially and functional outcome at 3 months, tested associations between clinical variables and structural imaging, several perfusion parameters and angiography.
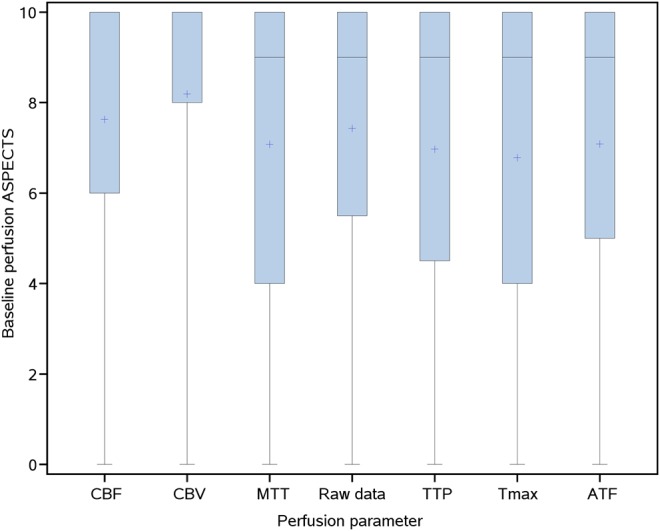
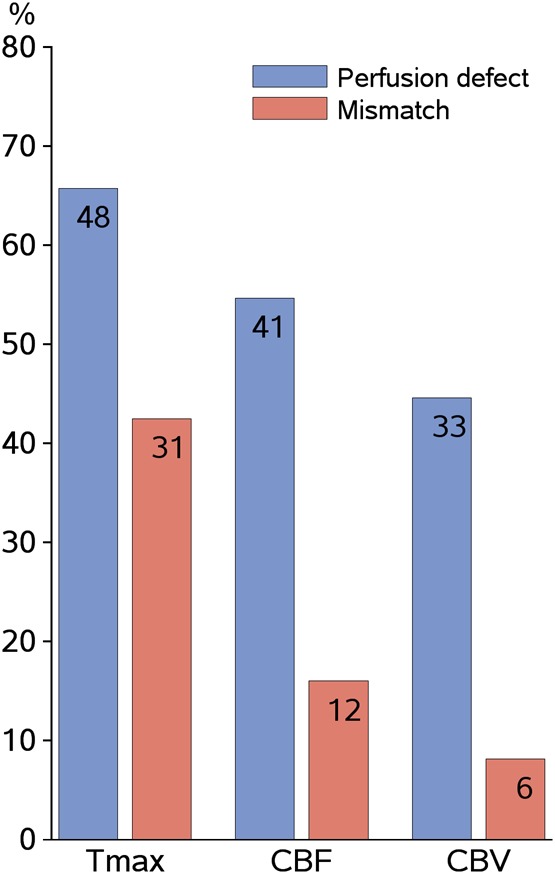
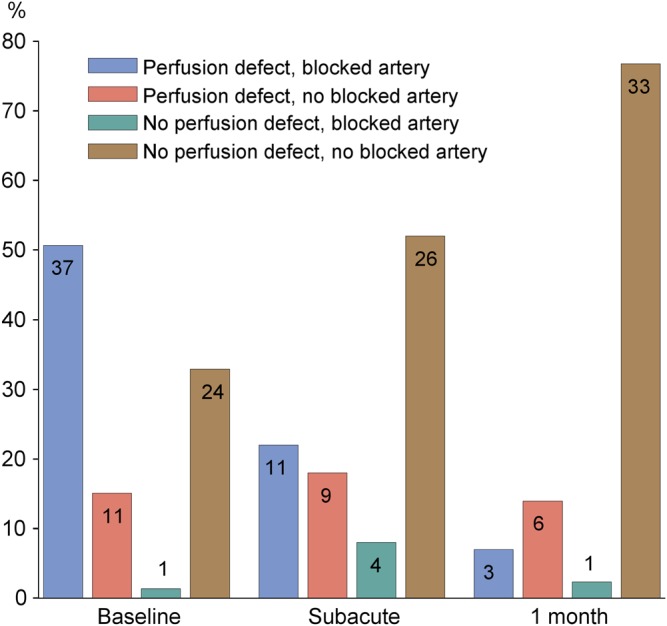
Results: Among 83 patients, median age 71 (maximum 89), median NIHSS 7 (range 1-30), 38 (46%) received alteplase, 41 (49%) had died or were dependent at 3 months. Most baseline imaging was CT (76%); follow-up was MR (79%) despite both being available acutely. At presentation, perfusion lesion size varied considerably between parameters (p<0.0001); 40 (48%) had arterial occlusion. Arterial occlusion and baseline perfusion lesion extent were both associated with baseline NIHSS (p<0.0001). Recanalisation by 72 h was associated with 1 month NIHSS (p=0.0007) and 3 month functional outcome (p=0.048), whereas tissue reperfusion, using even the best perfusion parameter, was not (p=0.11, p=0.08, respectively).
Conclusion: Early recanalisation on angiography appeared to predict clinical outcome more directly than did tissue reperfusion. Acute assessment with CT and follow-up with MR was practical and feasible, did not preclude image analysis, and would enhance trial recruitment and generalisability of results.
Keywords: Stroke.
Figures
Similar articles
-
Trial design and reporting standards for intra-arterial cerebral thrombolysis for acute ischemic stroke.Stroke. 2003 Aug;34(8):e109-37. doi: 10.1161/01.STR.0000082721.62796.09. Epub 2003 Jul 17. Stroke. 2003. PMID: 12869717
-
Arterial occlusion sites on magnetic resonance angiography influence the efficacy of intravenous low-dose (0.6 mg/kg) alteplase therapy for ischaemic stroke.Int J Stroke. 2009 Dec;4(6):425-31. doi: 10.1111/j.1747-4949.2009.00347.x. Int J Stroke. 2009. PMID: 19930051
-
Imaging perfusion deficits, arterial patency and thrombolysis safety and efficacy in acute ischaemic stroke. An observational study of the effect of advanced imaging methods in The Third International Stroke Trial (IST-3), a randomised controlled trial.Southampton (UK): NIHR Journals Library; 2014 Jul. Southampton (UK): NIHR Journals Library; 2014 Jul. PMID: 25642519 Free Books & Documents. Review.
-
National Institutes of Health stroke scale score and vessel occlusion in 2152 patients with acute ischemic stroke.Stroke. 2013 Apr;44(4):1153-7. doi: 10.1161/STROKEAHA.111.000604. Epub 2013 Mar 7. Stroke. 2013. PMID: 23471266
-
Computed tomography and magnetic resonance perfusion imaging in ischemic stroke: definitions and thresholds.Ann Neurol. 2011 Sep;70(3):384-401. doi: 10.1002/ana.22500. Epub 2011 Jul 27. Ann Neurol. 2011. PMID: 21796665 Review.
Cited by
-
Identification of imaging selection patterns in acute ischemic stroke patients and the influence on treatment and clinical trial enrollment decision making.Int J Stroke. 2016 Feb;11(2):180-90. doi: 10.1177/1747493015616634. Int J Stroke. 2016. PMID: 26783309 Free PMC article.
-
How many stroke patients might be eligible for mechanical thrombectomy?Eur Stroke J. 2016 Dec;1(4):264-271. doi: 10.1177/2396987316667176. Epub 2016 Aug 30. Eur Stroke J. 2016. PMID: 31008287 Free PMC article.
-
Utility of perfusion imaging in acute stroke treatment: a systematic review and meta-analysis.J Neurointerv Surg. 2017 Oct;9(10):1012-1016. doi: 10.1136/neurintsurg-2016-012751. Epub 2016 Nov 9. J Neurointerv Surg. 2017. PMID: 28899932 Free PMC article.
-
Acute Stroke Imaging Research Roadmap II.Stroke. 2013 Sep;44(9):2628-39. doi: 10.1161/STROKEAHA.113.002015. Epub 2013 Jul 16. Stroke. 2013. PMID: 23860298 Free PMC article. Review. No abstract available.
-
Clinical imaging in regenerative medicine.Nat Biotechnol. 2014 Aug;32(8):804-18. doi: 10.1038/nbt.2993. Nat Biotechnol. 2014. PMID: 25093889 Free PMC article. Review.
References
-
- Ebinger M, Christensen S, De Silva DA, et al. Expediting MRI-based proof-of-concept stroke trials using an earlier imaging end point. Stroke 2009;40:1353–8 - PubMed
-
- Rha J, Saver JL. The impact of recanalization on ischemic stroke outcome. A meta-analysis. Stroke 2007;38:967–73 - PubMed
-
- Davis SM, Donnan G, Parsons MW, et al. Effects of alteplase beyond 3 h after stroke in the Echoplanar Imaging Thrombolytic Evaluation Trial (EPITHET): a placebo-controlled radomised trial. Lancet Neurol 2008;7:299–309 - PubMed
-
- Mishra NK, Albers GW, Davis SM, et al. Mismatch-based delayed thrombolysis. A meta-analysis. Stroke 2010;41:e25–33 - PubMed
-
- Soares BP, Chien JD, Wintermark M. MT and CT monitoring of recanalization, reperfusion, and penumbra salvage. Everything that recanalizes does not necessarily reperfuse! Stroke 2009;40:S24–7 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical