

Clinical relevance and practical implications of trials of perfusion and angiographic imaging in patients with acute ischaemic stroke: a multicentre cohort imaging study
- PMID: 23644501
- PMCID: PMC3756443
- DOI: 10.1136/jnnp-2012-304807
Clinical relevance and practical implications of trials of perfusion and angiographic imaging in patients with acute ischaemic stroke: a multicentre cohort imaging study
Abstract
Background: In randomised trials testing treatments for acute ischaemic stroke, imaging markers of tissue reperfusion and arterial recanalisation may provide early response indicators.
Objective: To determine the predictive value of structural, perfusion and angiographic imaging for early and late clinical outcomes and assess practicalities in three comprehensive stroke centres.
Methods: We recruited patients with potentially disabling stroke in three stroke centres, performed magnetic resonance (MR) or CT, including perfusion and angiography imaging, within 6 h, at 72 h and 1 month after stroke. We assessed the National Institutes of Health Stroke Scale (NIHSS) score serially and functional outcome at 3 months, tested associations between clinical variables and structural imaging, several perfusion parameters and angiography.
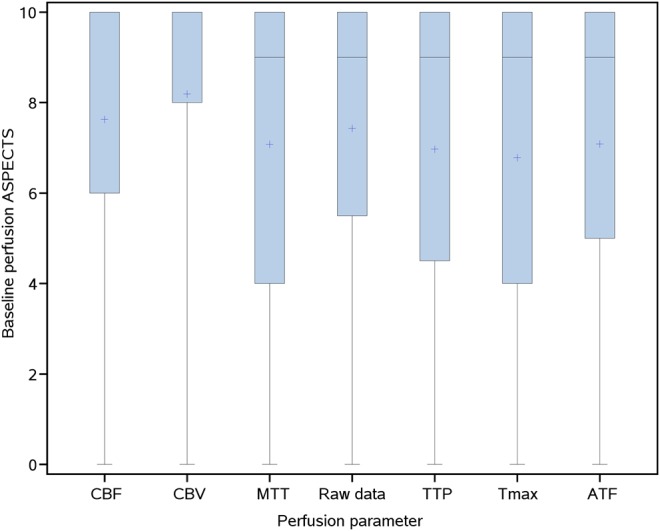
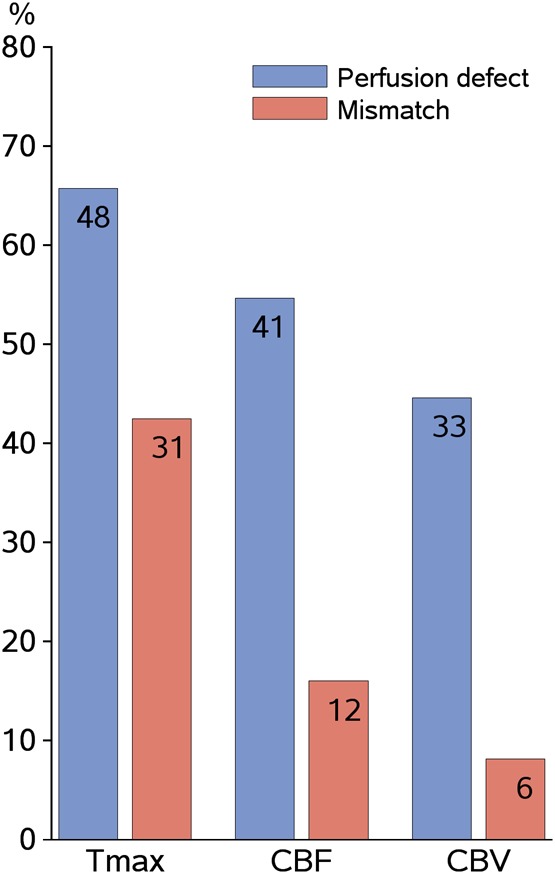
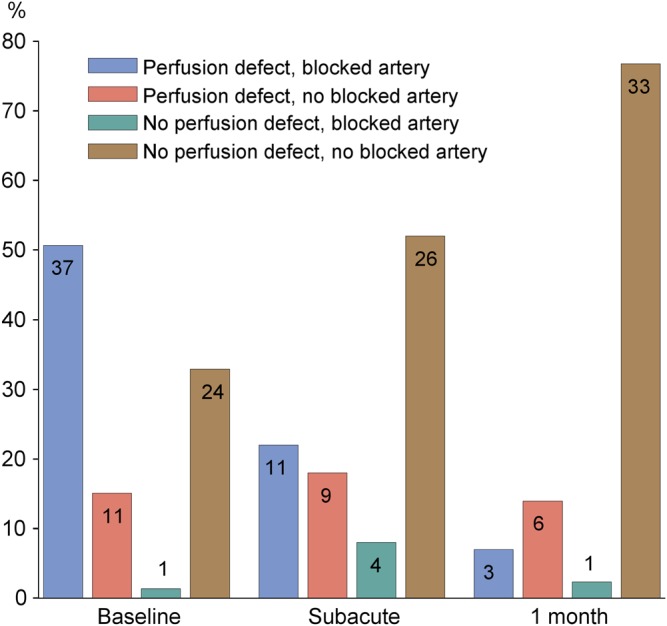
Results: Among 83 patients, median age 71 (maximum 89), median NIHSS 7 (range 1-30), 38 (46%) received alteplase, 41 (49%) had died or were dependent at 3 months. Most baseline imaging was CT (76%); follow-up was MR (79%) despite both being available acutely. At presentation, perfusion lesion size varied considerably between parameters (p<0.0001); 40 (48%) had arterial occlusion. Arterial occlusion and baseline perfusion lesion extent were both associated with baseline NIHSS (p<0.0001). Recanalisation by 72 h was associated with 1 month NIHSS (p=0.0007) and 3 month functional outcome (p=0.048), whereas tissue reperfusion, using even the best perfusion parameter, was not (p=0.11, p=0.08, respectively).
Conclusion: Early recanalisation on angiography appeared to predict clinical outcome more directly than did tissue reperfusion. Acute assessment with CT and follow-up with MR was practical and feasible, did not preclude image analysis, and would enhance trial recruitment and generalisability of results.
Keywords: Stroke.
Figures
References
-
- Ebinger M, Christensen S, De Silva DA, et al. Expediting MRI-based proof-of-concept stroke trials using an earlier imaging end point. Stroke 2009;40:1353–8 - PubMed
-
- Rha J, Saver JL. The impact of recanalization on ischemic stroke outcome. A meta-analysis. Stroke 2007;38:967–73 - PubMed
-
- Davis SM, Donnan G, Parsons MW, et al. Effects of alteplase beyond 3 h after stroke in the Echoplanar Imaging Thrombolytic Evaluation Trial (EPITHET): a placebo-controlled radomised trial. Lancet Neurol 2008;7:299–309 - PubMed
-
- Mishra NK, Albers GW, Davis SM, et al. Mismatch-based delayed thrombolysis. A meta-analysis. Stroke 2010;41:e25–33 - PubMed
-
- Soares BP, Chien JD, Wintermark M. MT and CT monitoring of recanalization, reperfusion, and penumbra salvage. Everything that recanalizes does not necessarily reperfuse! Stroke 2009;40:S24–7 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical