

Operative versus non-operative treatment for clavicle fracture: a meta-analysis
- PMID: 23645080
- PMCID: PMC3728389
- DOI: 10.1007/s00264-013-1871-z
Operative versus non-operative treatment for clavicle fracture: a meta-analysis
Abstract
Purpose: The purpose of this study was to assess the effects of operative and non-operative treatment on clavicle fractures.
Method: Relevant clinical trials on the operative and non-operative treatment for clavicle fractures were retrieved through searching the databases MEDLINE, Embase, OVID and the Cochrane Central Register of Controlled Trials up to December 2011. The quality of the included studies was assessed by two authors. A meta-analysis was carried out on homogeneous studies. Five studies involving 633 clavicle fractures were included.
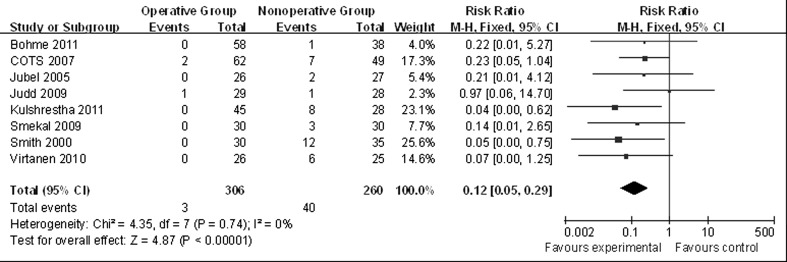
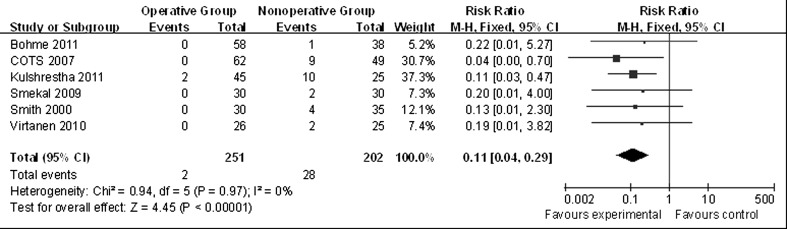
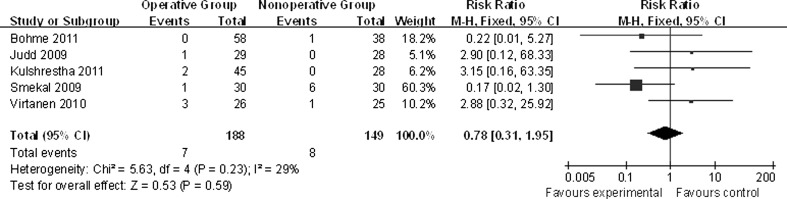
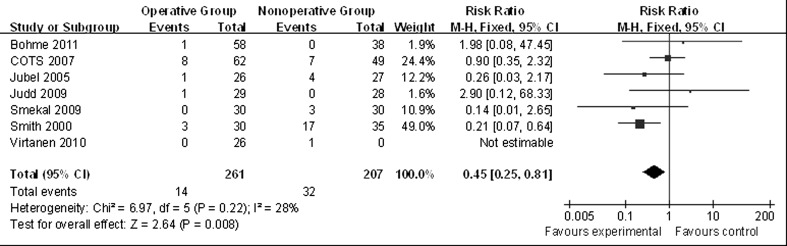
Results: The differences in nonunion [risk ratio (RR) 0.12, 95 % confidence interval (CI) 0.05-0.29], malunion (RR 0.11, 95 % CI 0.04-0.29) and neurological complications (RR 0.45, 95 % CI 0.25-0.81) were statistically significant between operative and non-operative treatment. There was no statistically significant difference in delayed union (RR 0.78, 95 % CI 0.31-1.95).
Conclusion: Operative treatment is better than non-operative treatment, but decisions should be made in accordance with specific conditions for clinical application.
Figures
Comment in
-
Comment on Liu et al.: Operative versus non-operative treatment for clavicle fracture: a meta-analysis.Int Orthop. 2013 Aug;37(8):1621. doi: 10.1007/s00264-013-1967-5. Epub 2013 Jun 18. Int Orthop. 2013. PMID: 23775456 Free PMC article. No abstract available.
-
Comment on Liu et al.: Operative versus non-operative treatment for clavicle fracture: a meta-analysis.Int Orthop. 2013 Aug;37(8):1619-20. doi: 10.1007/s00264-013-1969-3. Epub 2013 Jun 22. Int Orthop. 2013. PMID: 23793464 Free PMC article. No abstract available.
References
-
- Robinson CM, Court-Brown CM, McQueen MM, Wakefield AE. Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg Am. 2004;86(7):1359–1365. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
