

Long-term comparison of full-bed deep anterior lamellar keratoplasty and penetrating keratoplasty in treating keratoconus
- PMID: 23645180
- PMCID: PMC3650457
- DOI: 10.1631/jzus.B1200272
Long-term comparison of full-bed deep anterior lamellar keratoplasty and penetrating keratoplasty in treating keratoconus
Abstract
Objective: To compare postoperative outcomes of full-bed deep anterior lamellar keratoplasty (DALK) with penetrating keratoplasty (PK) in treating keratoconus.
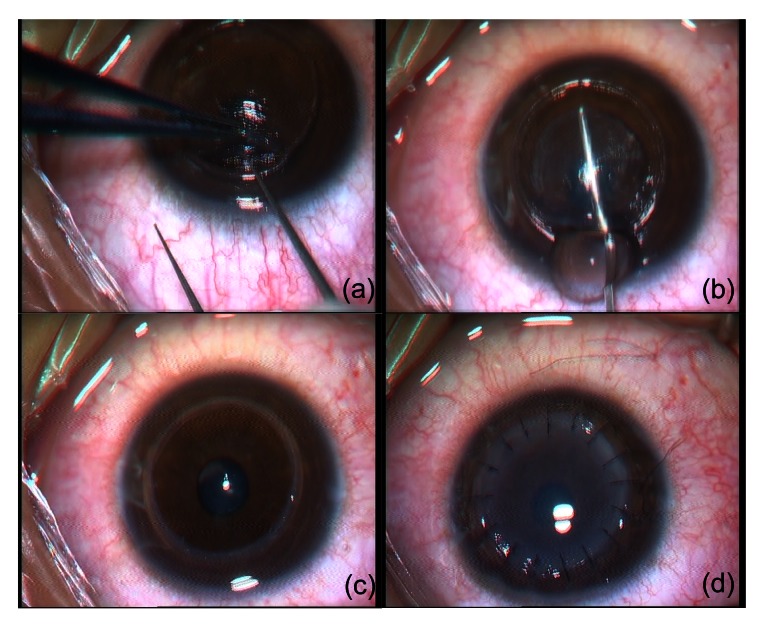
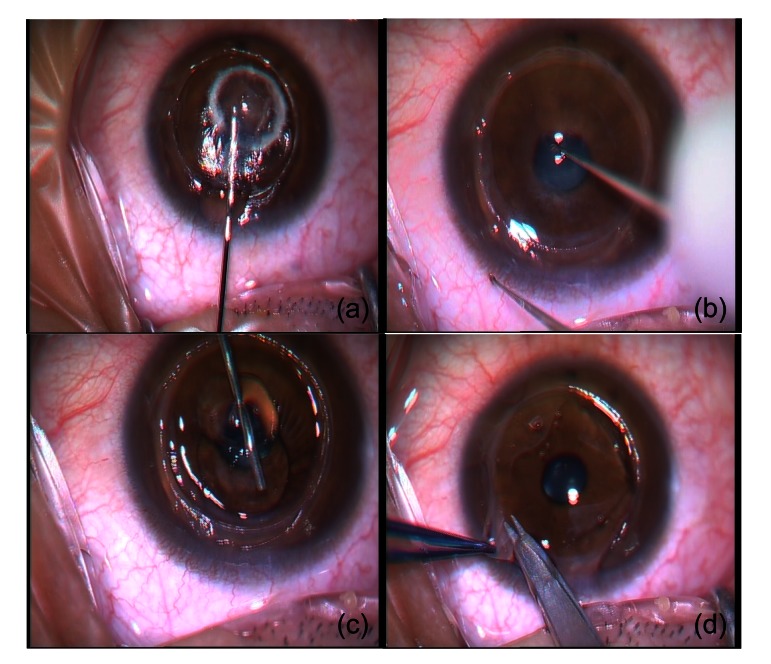
Methods: Seventy-five eyes of 64 patients who received full-bed DALK and 52 eyes of 51 patients who received PK between June 2000 and August 2010 were included in this retrospective study. Full-bed DALK was performed using Yao's hooking-detaching technique. PK was performed using a standard technique. Intraoperative and postoperative complications, visual acuity, rejection, graft survival, endothelial cell density, corneal sensation recovery, and re-innervation were compared between the two groups.
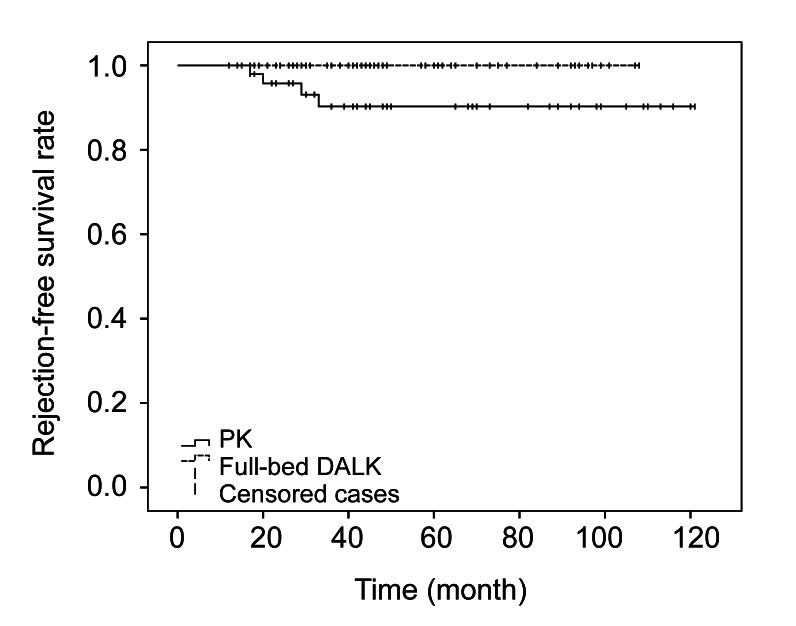
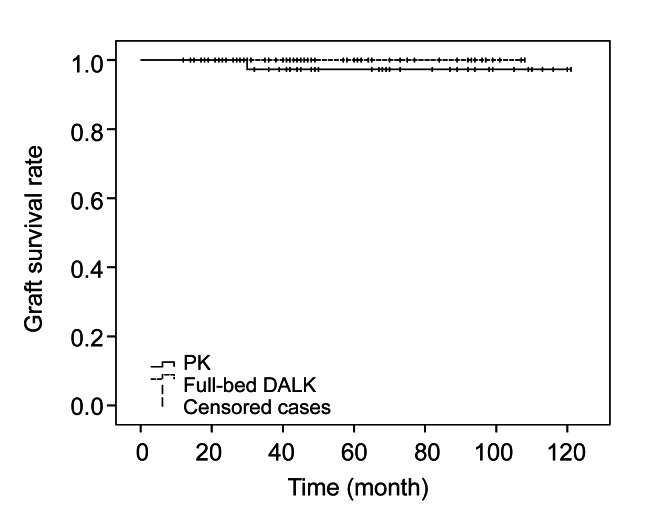
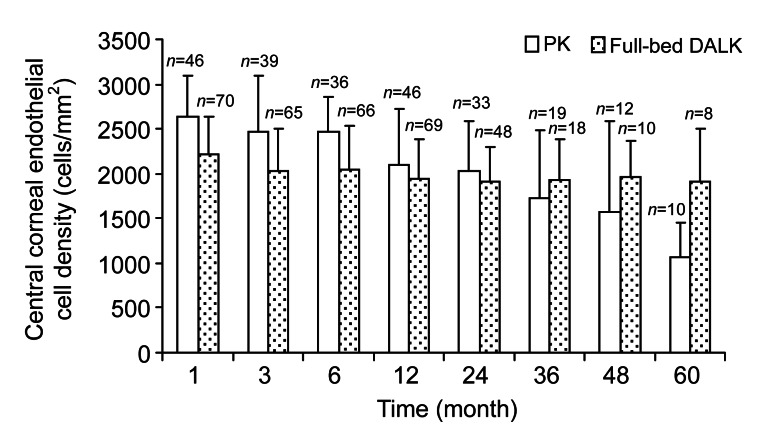
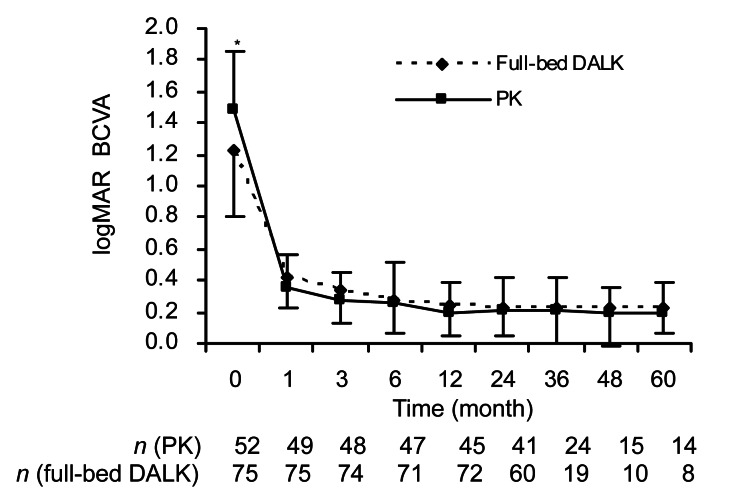
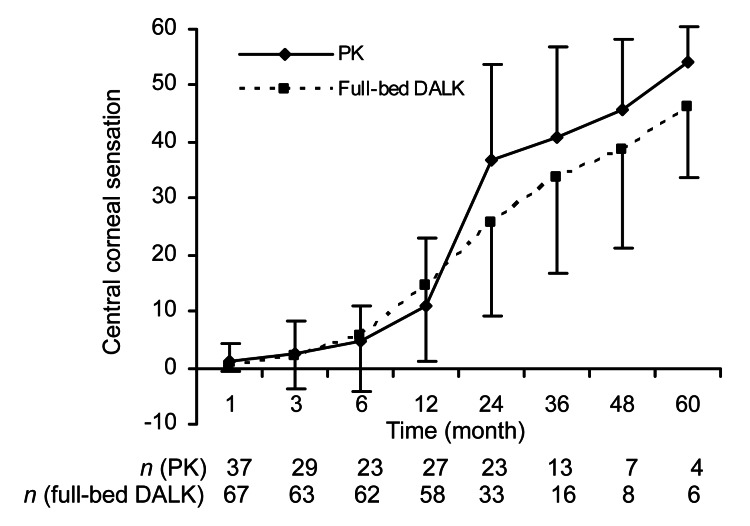
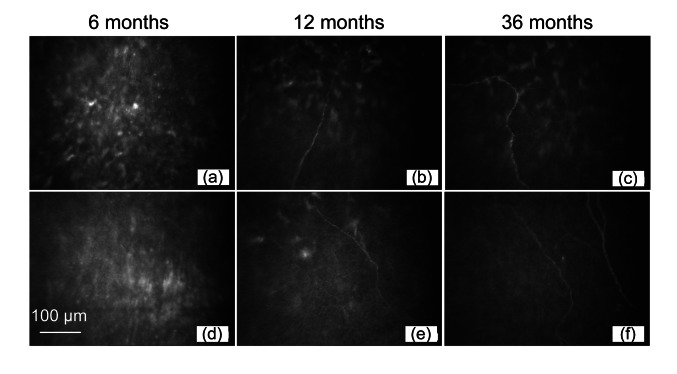
Results: A best correct visual acuity of 0.5 or better was achieved in 90.7% of eyes after full-bed DALK and in 92.3% of eyes after PK (P=0.75). By the fifth postoperative year, graft endothelial cell loss reached 34.6% in the PK group vs. 13.9% in the full-bed DALK group (P<0.001). There were no statistical differences in corneal sensitivity recovery or corneal re-innervation between the groups (P>0.05). Intraoperative microperforation occurred in seven out of 75 (9.3%) eyes with a temporally postoperative double anterior chamber in two eyes in the full-bed DALK group. Postoperative complications in the PK vs. the full-bed DALK groups respectively were: rejection (7.7% vs. 0%, P=0.015), high intraocular pressure (IOP) (46.2% vs. 1.3%, P<0.001), secondary glaucoma (9.6% vs. 0%, P=0.006), complicated cataract (19.2% vs. 0%, P<0.001), and wound dehiscence (9.6% vs. 0%, P=0.006).
Conclusions: Both full-bed DALK and PK can offer long-term satisfactory visual outcomes for keratoconus. Graft rejection, secondary glaucoma, complicated cataracts, and constant endothelial cell loss were observed in eyes only after PK.
Conflict of interest statement
All procedures followed were in accordance with the ethical standards of the Ethics Committee of Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, China and with the Helsinki Declaration of 1975, as revised in 2000(5). Informed consent was obtained from all patients for being included in the study.
Figures
Similar articles
-
Comparative study of keratoconus between Anwar's deep anterior lamellar keratoplasty versus converted penetrating keratoplasty.Arch Soc Esp Oftalmol. 2015 Jun;90(6):257-63. doi: 10.1016/j.oftal.2014.11.008. Epub 2015 Mar 25. Arch Soc Esp Oftalmol. 2015. PMID: 25817955 English, Spanish.
-
Systematic review comparing penetrating keratoplasty and deep anterior lamellar keratoplasty for management of keratoconus.Cont Lens Anterior Eye. 2017 Feb;40(1):3-14. doi: 10.1016/j.clae.2016.10.001. Epub 2016 Oct 29. Cont Lens Anterior Eye. 2017. PMID: 27802912
-
Penetrating Keratoplasty Versus Deep Anterior Lamellar Keratoplasty in Children and Adolescents With Keratoconus.Am J Ophthalmol. 2021 Jun;226:13-21. doi: 10.1016/j.ajo.2021.01.010. Epub 2021 Jan 30. Am J Ophthalmol. 2021. PMID: 33529592
-
Comparison of outcomes of lamellar keratoplasty and penetrating keratoplasty in keratoconus.Am J Ophthalmol. 2009 Nov;148(5):744-751.e1. doi: 10.1016/j.ajo.2009.05.028. Epub 2009 Jul 9. Am J Ophthalmol. 2009. PMID: 19589495
-
Deep anterior lamellar keratoplasty as an alternative to penetrating keratoplasty a report by the american academy of ophthalmology.Ophthalmology. 2011 Jan;118(1):209-18. doi: 10.1016/j.ophtha.2010.11.002. Ophthalmology. 2011. PMID: 21199711 Review.
Cited by
-
Donor and Recipient Sex Matching and Corneal Graft Failure in High-Risk and Non-High-Risk Patients.J Ophthalmol. 2022 Apr 16;2022:1520912. doi: 10.1155/2022/1520912. eCollection 2022. J Ophthalmol. 2022. PMID: 35469216 Free PMC article.
-
Small-Incision Femtosecond Laser-Assisted Intracorneal Concave Lenticule Implantation in Patients With Keratoconus.Cornea. 2019 Apr;38(4):446-453. doi: 10.1097/ICO.0000000000001877. Cornea. 2019. PMID: 30840609 Free PMC article.
-
Current techniques of lamellar keratoplasty for keratoconus.Saudi Med J. 2016 Feb;37(2):127-36. doi: 10.15537/smj.2016.2.12985. Saudi Med J. 2016. PMID: 26837393 Free PMC article. Review.
-
Efficacy and safety of deep anterior lamellar keratoplasty vs. penetrating keratoplasty for keratoconus: a meta-analysis.PLoS One. 2015 Jan 29;10(1):e0113332. doi: 10.1371/journal.pone.0113332. eCollection 2015. PLoS One. 2015. PMID: 25633311 Free PMC article.
-
Corneal surgery in keratoconus: which type, which technique, which outcomes?Eye Vis (Lond). 2016 Jan 18;3:2. doi: 10.1186/s40662-016-0033-y. eCollection 2016. Eye Vis (Lond). 2016. PMID: 26783544 Free PMC article. Review.
References
-
- Al-Torbak AA, Al-Motowa S, Al-Assiri A, Al-Kharashi S, Al-Shahwan S, Al-Mezaine H, Teichmann K. Deep anterior lamellar keratoplasty for keratoconus. Cornea. 2006;25(4):408–412. - PubMed
-
- Amayem AF, Anwar M. Fluid lamellar keratoplasty in keratoconus. Ophthalmology. 2000;107(1):76–79. discussion 80. - PubMed
-
- Cheng YY, Visser N, Schouten JS, Wijdh RJ, Pels E, van Cleynenbreugel H, Eggink CA, Zaal MJ, Rijneveld WJ, Nuijts RM. Endothelial cell loss and visual outcome of deep anterior lamellar keratoplasty versus penetrating keratoplasty: a randomized multicenter clinical trial. Ophthalmology. 2011;118(2):302–309. doi: 10.1016/j.ophtha.2010.06.005. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
