

Lutein/zeaxanthin for the treatment of age-related cataract: AREDS2 randomized trial report no. 4
- PMID: 23645227
- PMCID: PMC6774801
- DOI: 10.1001/jamaophthalmol.2013.4412
Lutein/zeaxanthin for the treatment of age-related cataract: AREDS2 randomized trial report no. 4
Abstract
Importance: Age-related cataract is a leading cause of visual impairment in the United States. The prevalence of age-related cataract is increasing, with an estimated 30.1 million Americans likely to be affected by 2020.
Objective: To determine whether daily oral supplementation with lutein/zeaxanthin affects the risk for cataract surgery.
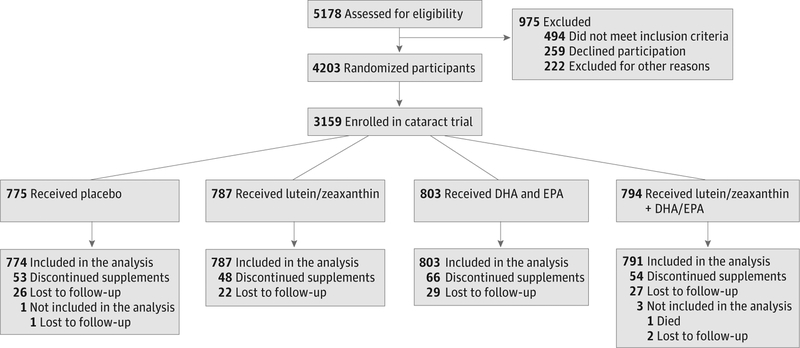
Design, setting, and patients: The Age-Related Eye Disease Study 2 (AREDS2), a multicenter, double-masked clinical trial, enrolled 4203 participants, aged 50 to 85 years, at risk for progression to advanced age-related macular degeneration.
Interventions: Participants were randomly assigned to daily placebo; lutein/zeaxanthin, 10mg/2mg; omega-3 long-chain polyunsaturated fatty acids, 1 g; or a combination to evaluate the effects on the primary outcome of progression to advanced age-related macular degeneration.
Main outcomes and measures: Cataract surgery was documented at annual study examination with the presence of pseudophakia or aphakia, or reported during telephone calls at 6-month intervals between study visits. Annual best-corrected visual acuity testing was performed. A secondary outcome of AREDS2 was to evaluate the effects of lutein/zeaxanthin on the subsequent need for cataract surgery.
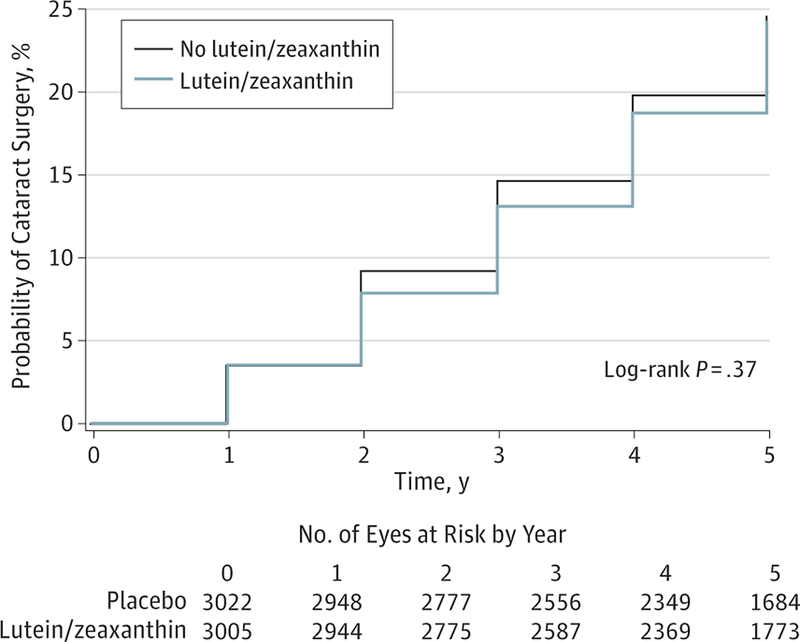
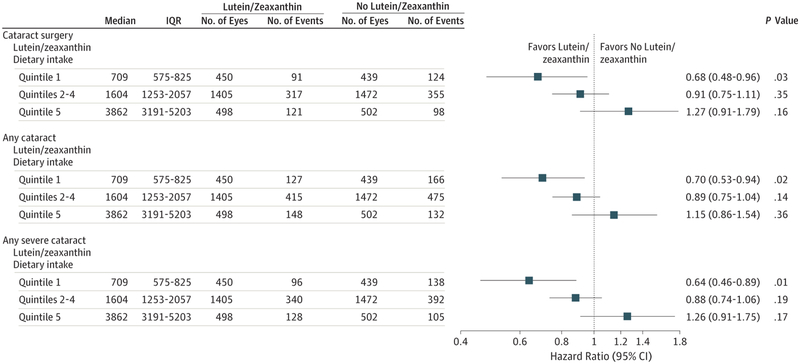
Results: A total of 3159 AREDS2 participants were phakic in at least 1 eye and 1389 of 6027 study eyes underwent cataract surgery during the study, with median follow-up of 4.7 years. The 5-year probability of progression to cataract surgery in the no lutein/zeaxanthin group was 24%. For lutein/zeaxanthin vs no lutein/zeaxanthin, the hazard ratios for progression to cataract surgery was 0.96 (95% CI, 0.84-1.10; P = .54). For participants in the lowest quintile of dietary intake of lutein/zeaxanthin, the hazard ratio comparing lutein/zeaxanthin vs no lutein/zeaxanthin for progression to cataract surgery was 0.68 (95% CI, 0.48-0.96; P = .03). The hazard ratio for 3 or more lines of vision loss was 1.03 (95% CI, 0.93-1.13; P = .61 for lutein/zeaxanthin vs no lutein/zeaxanthin).
Conclusions and relevance: Daily supplementation with lutein/zeaxanthin had no statistically significant overall effect on rates of cataract surgery or vision loss.
Trial registration: clinicaltrials.gov Identifier: NCT00345176.
Conflict of interest statement
Figures

References
-
- Pascolini D, Mariotti SP, Pokharel GP, et al. 2002 global update of available data on visual impairment: a compilation of population-based prevalence studies. Ophthalmic Epidemiol. 2004;11(2):67–115. - PubMed
-
- Congdon N, O’Colmain B, Klaver CC, et al. ; Eye Diseases Prevalence Research Group. Causes and prevalence of visual impairment among adults in the United States. Arch Ophthalmol. 2004;122(4):477–485. - PubMed
-
- Congdon N, Vingerling JR, Klein BE, et al. ; Eye Diseases Prevalence Research Group. Prevalence of cataract and pseudophakia/aphakia among adults in the United States. Arch Ophthalmol. 2004;122(4):487–494. - PubMed
-
- Leske MC, Chylack LT Jr, Wu SY. The Lens Opacities Case-Control Study: risk factors for cataract. Arch Ophthalmol. 1991;109(2):244–251. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
