

Reliability and validity of measuring acetabular component orientation by plain anteroposterior radiographs
- PMID: 23645336
- PMCID: PMC3734435
- DOI: 10.1007/s11999-013-3021-8
Reliability and validity of measuring acetabular component orientation by plain anteroposterior radiographs
Abstract
Background: Inaccurate placement of an acetabular cup can cause impingement, dislocation, and accelerated wear. However, there is no universally agreed-on approach to measuring cup position using plain radiographs.
Objectives/purposes: Our goal was to evaluate the reliability and validity of measuring the orientation of acetabular components on plain anteroposterior (AP) radiographs.
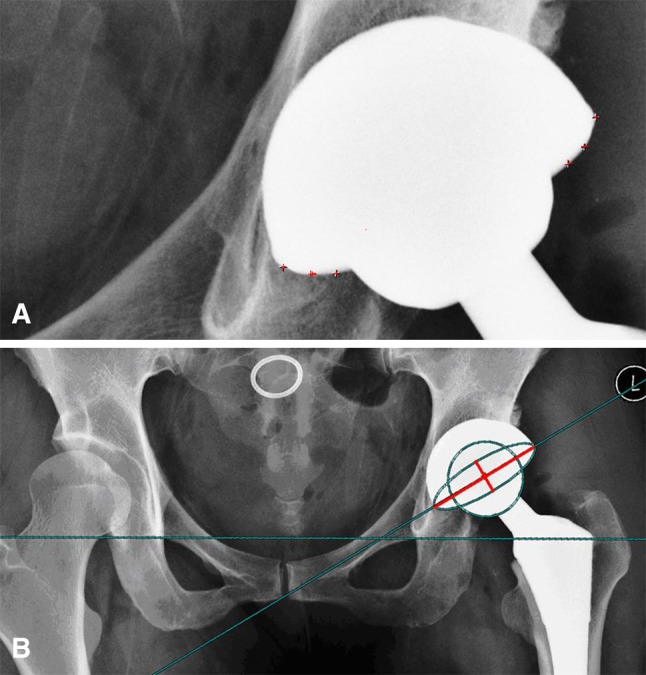
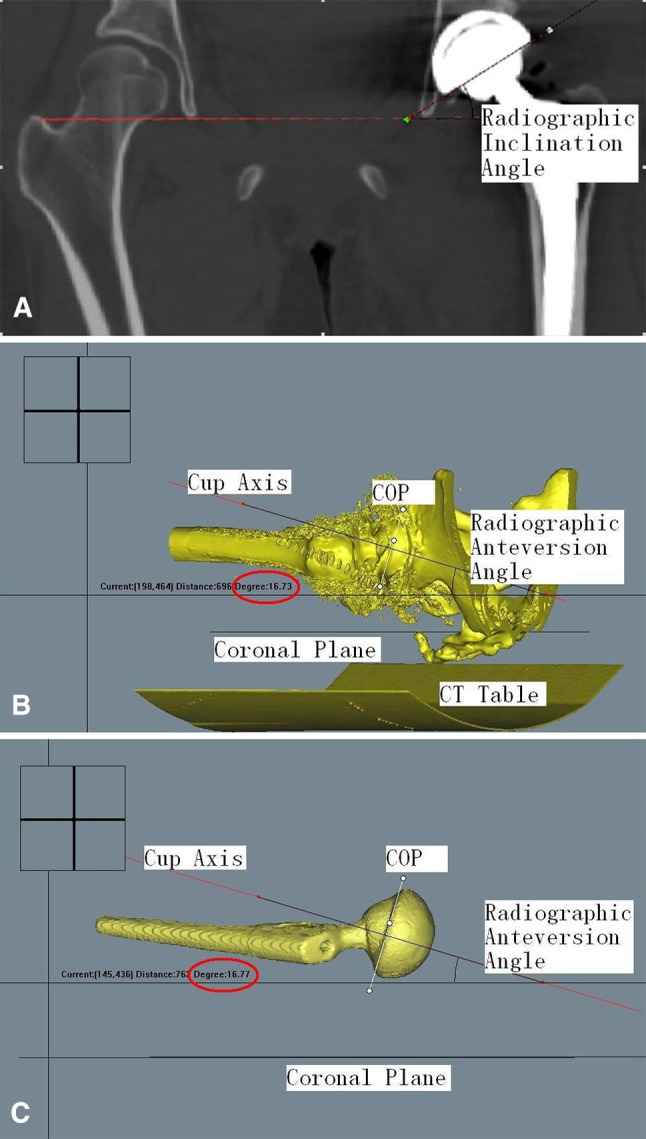
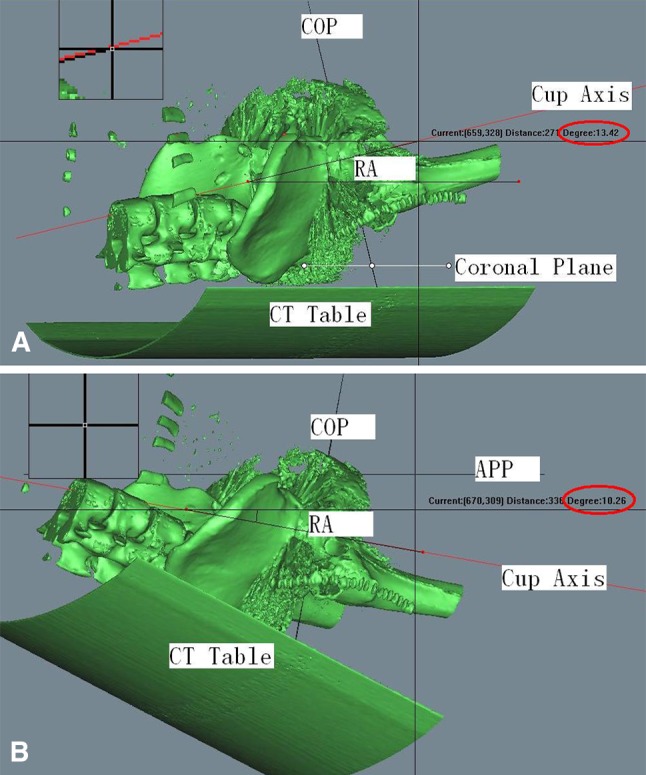
Methods: We obtained plain AP radiographs and CT scans for 60 patients who underwent 60 primary total hip arthroplasties (THAs). The method devised by Lewinnek et al. was used to measure the orientation of acetabular components on plain AP radiographs, and three-dimensional (3-D) CT scans were used to measure both the radiographic anteversion angle and the inclination angle. Reliability was evaluated by analysis of the agreement between inter- and intraobserver measurements using plain AP radiographs. Measurements on 3-D CT scans were regarded as the reference standard; validity was assessed by comparing radiographic measurements with the CT scans.
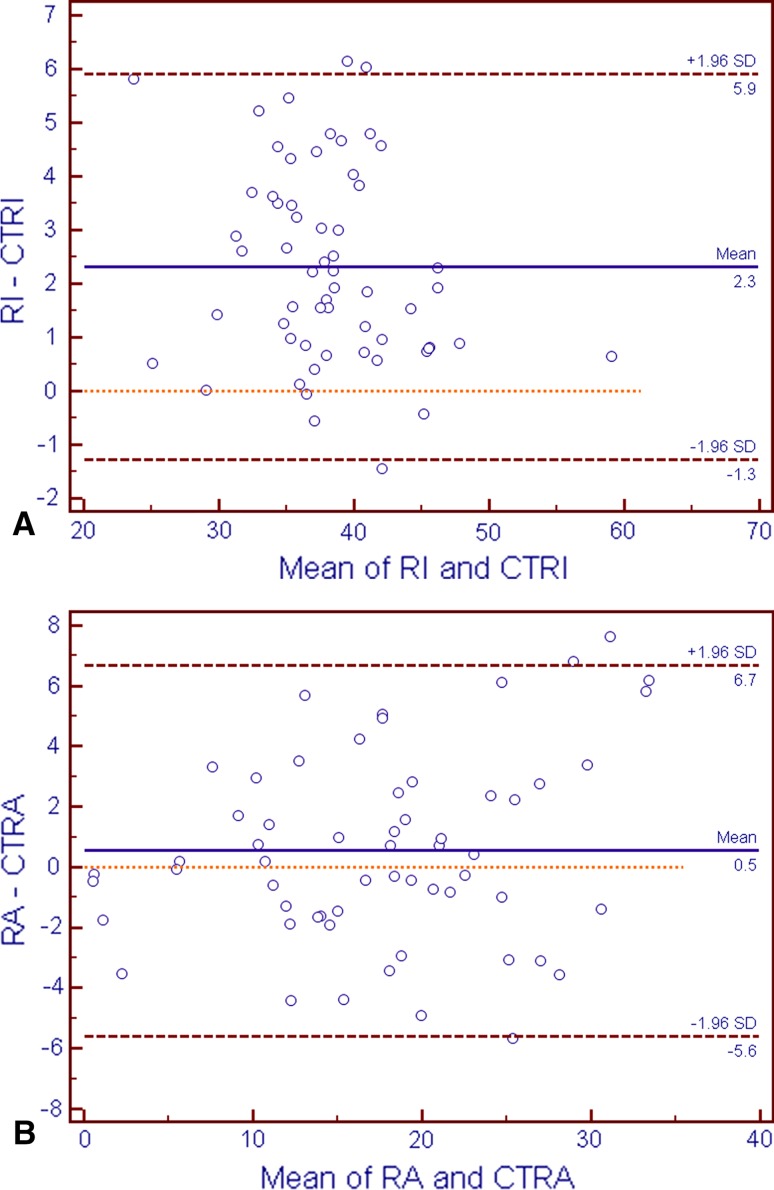
Results: Inter- and intraobserver reliability for measuring component orientation on plain AP radiographs was nearly perfect with intraclass correlation coefficients of 0.896 and 0.969 for anteversion and 0.984 and 0.993 for inclination. Measurement of cup inclination angles differed between plain radiographs and CT scans, but the difference was small, and the difference, although statistically significant, probably was not clinically important (2.3° ± 1.8°, p < 0.001). There was no significant difference between the anteversion as measured on CT scan versus that measured on plain radiographs (p = 0.19).
Conclusions: Measurement of the orientation of acetabular components on plain AP radiographs is reliable and accurate compared with measurement on CT.
Figures
References
-
- Ackland MK, Bourne WB, Uhthoff HK. Anteversion of the acetabular cup: measurement of angle after total hip replacement. J Bone Joint Surg Br. 1986;68:409–413. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
