

Preemptive low-dose dexamethasone reduces postoperative emesis and pain after TKA: a randomized controlled study
- PMID: 23645340
- PMCID: PMC3734432
- DOI: 10.1007/s11999-013-3032-5
Preemptive low-dose dexamethasone reduces postoperative emesis and pain after TKA: a randomized controlled study
Abstract
Background: Dexamethasone is a potent analgesic and antiemetic. However, the benefit of dexamethasone after TKA is unclear, as is the efficacy in a current multimodal regime.
Questions/purposes: We determined (1) whether the addition of dexamethasone to a protocol including ramosetron further reduces postoperative emesis compared with ramosetron alone; (2) whether it reduces postoperative pain; and (3) whether it increases the risk for wound complications in a current multimodal regime after TKA.
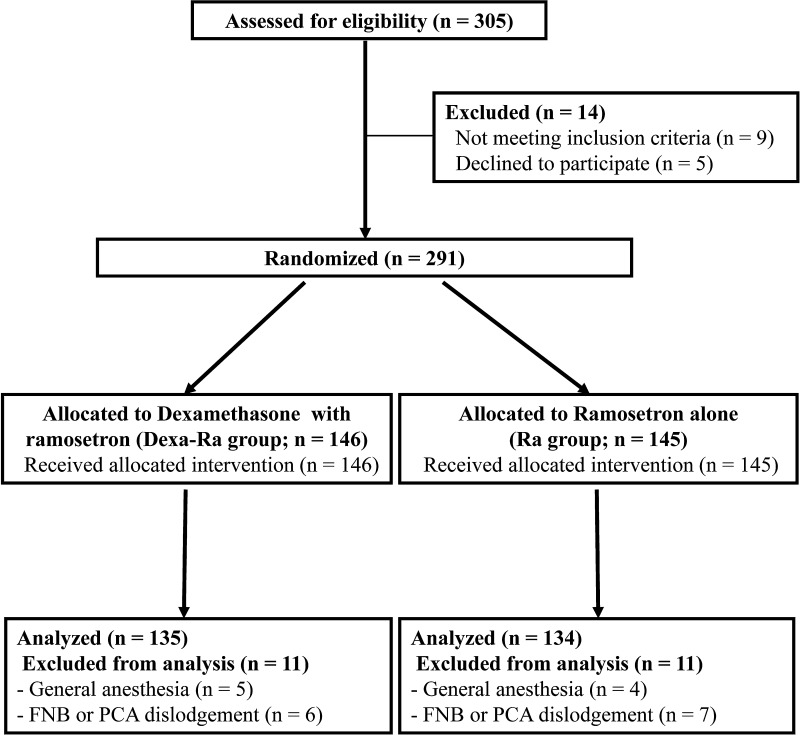
Methods: We randomized 269 patients undergoing TKAs to receive dexamethasone (10 mg) 1 hour before surgery and ramosetron immediately after surgery (Dexa-Ra group, n = 135), or ramosetron alone (Ra group, n = 134). We recorded the incidence of postoperative nausea and vomiting (PONV), severity of nausea, incidence of antiemetic requirement, complete response, pain level, and opioid consumption. Patients were assessed 0 to 6, 6 to 24, 24 to 48, and 48 to 72 hours postoperatively. In addition, patients were evaluated for wound complications and periprosthetic joint infections at a minimum of 1 year after surgery.
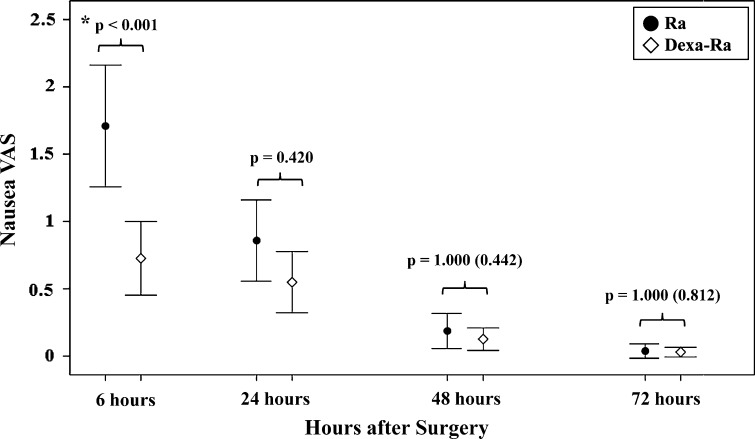
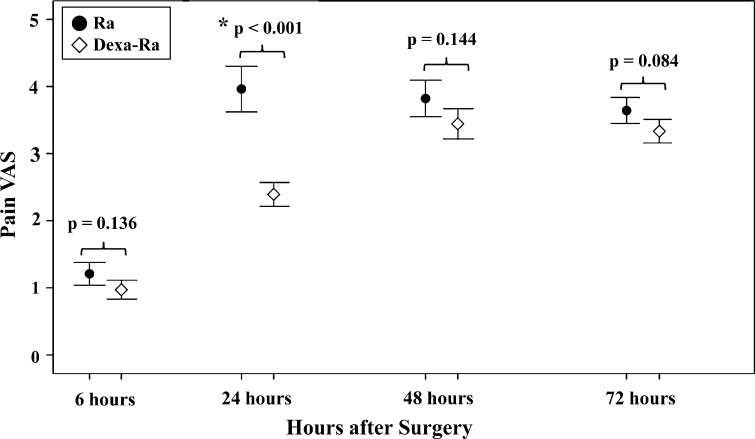
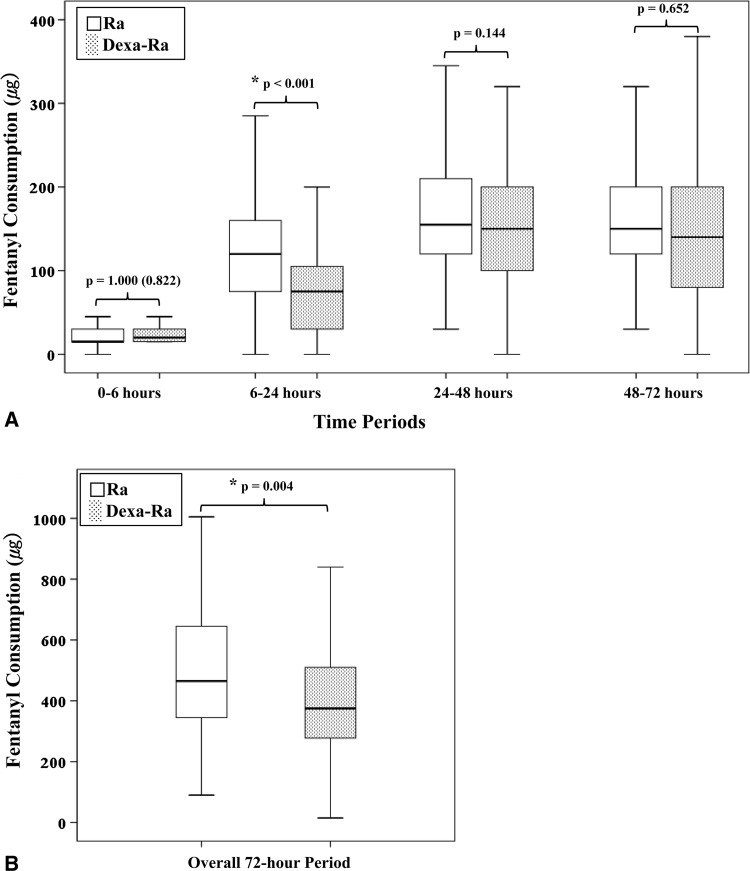
Results: The Dexa-Ra group had a lower incidence of PONV during the entire 72-hour evaluation period and experienced less severe nausea for the first 6 hours after TKA, although not between 6 to 72 hours. Overall use of a rescue antiemetic was less frequent, and complete response was more frequent in the Dexa-Ra group. Patients in the Dexa-Ra group experienced lower pain and consumed less opioids during the 6- to 24-hour period and during the overall study period. No differences were found in wound complications between the groups, and each group had one case of periprosthetic joint infection.
Conclusions: Patients who received prophylactic dexamethasone in addition to ramosetron had reduced postoperative emesis and pain without increased risks for wound complications, compared with patients who received ramosetron alone in patients managed using a multimodal regimen after TKA.
Figures
References
-
- Aminmansour B, Khalili HA, Ahmadi J, Nourian M. Effect of high-dose intravenous dexamethasone on postlumbar discectomy pain. Spine (Phila Pa 1976). 2006;31:2415–2417. - PubMed
-
- Apfel CC, Korttila K, Abdalla M, Kerger H, Turan A, Vedder I, Zernak C, Danner K, Jokela R, Pocock SJ, Trenkler S, Kredel M, Biedler A, Sessler DI, Roewer N. A factorial trial of six interventions for the prevention of postoperative nausea and vomiting. N Engl J Med. 2004;350:2441–2451. doi: 10.1056/NEJMoa032196. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
