

The quality of quality measures: HEDIS® quality measures for medication management in the elderly and outcomes associated with new exposure
- PMID: 23645530
- PMCID: PMC3720786
- DOI: 10.1007/s40266-013-0086-8
The quality of quality measures: HEDIS® quality measures for medication management in the elderly and outcomes associated with new exposure
Abstract
Background: Clinical validation studies of the Healthcare Effectiveness Data and Information Set (HEDIS®) measures of inappropriate prescribing in the elderly are limited.
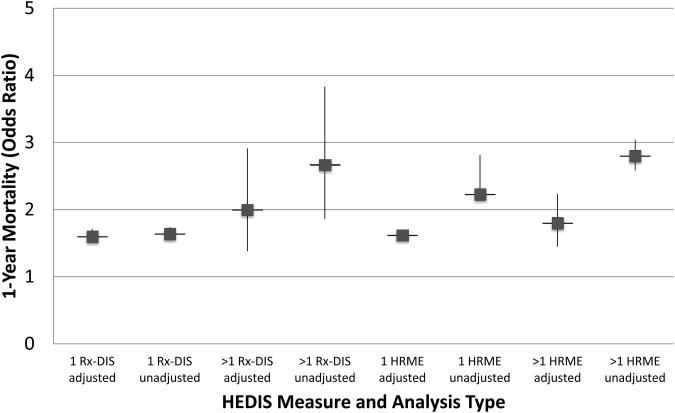
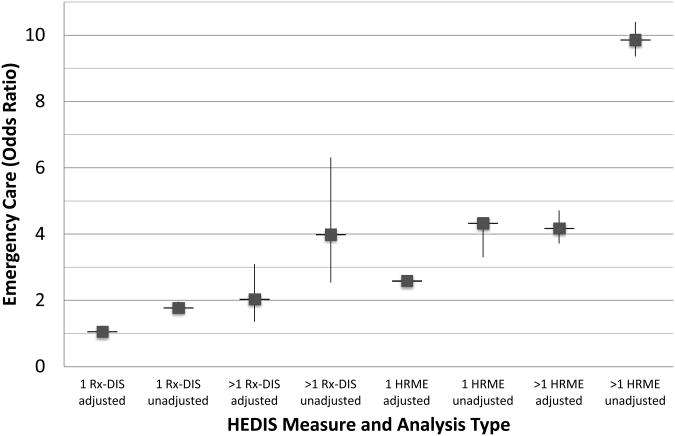
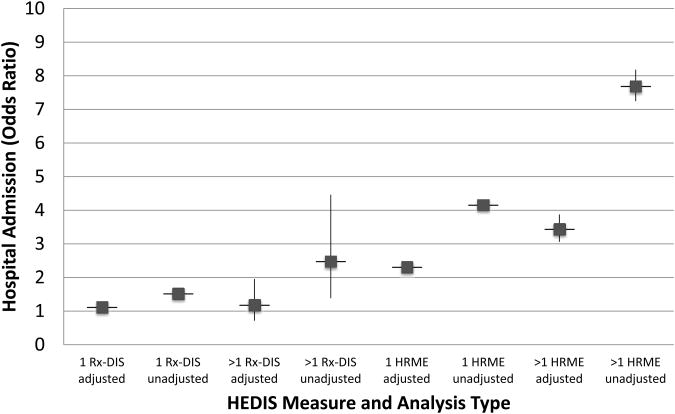
Objectives: The objective of this study was to examine associations of new exposure to high-risk medication in the elderly (HRME) and drug-disease interaction (Rx-DIS) with mortality, hospital admission, and emergency care.
Methods: A retrospective database study was conducted examining new use of HRME and Rx-DIS in fiscal year 2006 (Oct 2005-Sep 2006; FY06), with index date being the date of first HRME/Rx-DIS exposure, or first day of FY07 if no HRME/Rx-DIS exposure. Outcomes were assessed 1 year after the index date. The participants were veterans who were ≥65 years old in FY06 and received Veterans Health Administration (VA) care in FY05-06. A history of falls/hip fracture, chronic renal failure, and/or dementia per diagnosis codes defined the Rx-DIS subsample. The variables included a number of new unique HRME drug exposures and new unique Rx-DIS drug exposure (0, 1, >1) in FY06, and outcomes (i.e., 1-year mortality, hospital admission, and emergency care) up to 1 year after exposure. Descriptive statistics summarized variables for the overall HRME cohort and the Rx-DIS subset. Multivariable statistical analyses using generalized estimating equations (GEE) models with a logit link accounted for nesting of patients within facilities. For these latter analyses, we controlled for demographic characteristics, chronic disease states, and indicators of disease burden the previous year (e.g., number of prescriptions, emergency/hospital care).
Results: Among the 1,807,404 veterans who met inclusion criteria, 5.2 % had new HRME exposure. Of the 256,388 in the Rx-DIS cohort, 3.6 % had new Rx-DIS exposure. Multivariable analyses found that HRME was significantly associated with mortality [1: adjusted odds ratio (AOR) = 1.62, 95 % CI 1.56-1.68; >1: AOR = 1.80, 95 % CI 1.45-2.23], hospital admission (1: AOR = 2.31, 95 % CI 2.22-2.40; >1: AOR = 3.44, 95 % CI 3.06-3.87), and emergency care (1: AOR = 2.59, 95 % CI 2.49-2.70; >1: AOR = 4.18, 95 % CI 3.71-4.71). Rx-DIS exposure was significantly associated with mortality (1: AOR = 1.60, 95 % CI 1.51-1.71; >1: AOR = 2.00, 95 % CI 1.38-2.91), hospital admission for one exposure (1: AOR = 1.12, 95 % CI 1.03-1.27; >1: AOR = 1.18, 95 % CI 0.71-1.95), and emergency care for two or more exposures (1: AOR = 1.06, 95 % CI 0.97-1.15; >1: AOR = 2.0, 95 % CI 1.35-3.10).
Conclusions: Analyses support the link between HRME/Rx-DIS exposure and clinically significant outcomes in older veterans. Now is the time to begin incorporating input from both patients who receive these medications and providers who prescribe to develop approaches to reduce exposure to these agents.
Figures
Similar articles
-
Facility-level variation in potentially inappropriate prescribing for older veterans.J Am Geriatr Soc. 2012 Jul;60(7):1222-9. doi: 10.1111/j.1532-5415.2012.04042.x. Epub 2012 Jun 21. J Am Geriatr Soc. 2012. PMID: 22726206 Free PMC article.
-
Assessment of Clinical Pharmacy Interventions to Reduce Outpatient Use of High-Risk Medications in the Elderly.J Manag Care Spec Pharm. 2017 May;23(5):520-524. doi: 10.18553/jmcp.2017.23.5.520. J Manag Care Spec Pharm. 2017. PMID: 28448781 Free PMC article.
-
Exposure to potentially harmful drug-disease interactions in older community-dwelling veterans based on the Healthcare Effectiveness Data and Information Set quality measure: who is at risk?J Am Geriatr Soc. 2011 Sep;59(9):1673-8. doi: 10.1111/j.1532-5415.2011.03524.x. Epub 2011 Aug 10. J Am Geriatr Soc. 2011. PMID: 21831166 Free PMC article.
-
Early detection of carcinoma: correlating quantifiable tumor biomarkers with High-Resolution Microscopy (HRME) findings.Expert Rev Mol Diagn. 2025 Jan-Mar;25(1-3):33-45. doi: 10.1080/14737159.2025.2451717. Epub 2025 Jan 11. Expert Rev Mol Diagn. 2025. PMID: 39778093 Review.
-
Therapeutic Protein Drug Interactions: A White Paper From the International Consortium for Innovation and Quality in Pharmaceutical Development.Clin Pharmacol Ther. 2023 Jun;113(6):1185-1198. doi: 10.1002/cpt.2814. Epub 2023 Jan 17. Clin Pharmacol Ther. 2023. PMID: 36477720 Review.
Cited by
-
Tools for Assessment of the Appropriateness of Prescribing and Association with Patient-Related Outcomes: A Systematic Review.Drugs Aging. 2018 Jan;35(1):43-60. doi: 10.1007/s40266-018-0516-8. Drugs Aging. 2018. PMID: 29350335
-
Quality Improvement Project to Reduce Drug-Related Problems (DRPs) and Potentially Inappropriate Medications (PIMs) in Geriatrics Cardiac Clinic in Saudi Arabia.Can Geriatr J. 2019 Jun 30;22(2):49-54. doi: 10.5770/cgj.22.338. eCollection 2019 Jun. Can Geriatr J. 2019. PMID: 31258827 Free PMC article.
-
Explaining Improved Use of High-Risk Medications in Medicare Between 2007 and 2011.J Am Geriatr Soc. 2016 Mar;64(3):674-6. doi: 10.1111/jgs.14000. J Am Geriatr Soc. 2016. PMID: 27000357 Free PMC article. No abstract available.
-
Effect of hospitalization on inappropriate prescribing in elderly Medicare beneficiaries.J Am Geriatr Soc. 2015 Apr;63(4):699-707. doi: 10.1111/jgs.13318. Epub 2015 Apr 8. J Am Geriatr Soc. 2015. PMID: 25855518 Free PMC article.
-
Association of Potentially Inappropriate Medication Classes with Mortality Risk Among Older Adults Initiating Hemodialysis.Drugs Aging. 2023 Aug;40(8):741-749. doi: 10.1007/s40266-023-01039-z. Epub 2023 Jun 28. Drugs Aging. 2023. PMID: 37378815 Free PMC article.
References
-
- Institute of Medicine To err is human: building a safer health system. Washington, DC: National Academies Press; 1999. - PubMed
-
- Wenger NS, Young RT. Quality indicators for continuity and coordination of care in vulnerable elders. J Am Geriatr Soc. 2007;55(s2):S285–S92. - PubMed
-
- Brook RH, McGlynn EA, Shekelle PG. Defining and measuring quality of care: a perspective from US researchers. Qual Assur Health Care. 2000;12(4):281–95. - PubMed
-
- Beers MH, Ouslander JG, Rollingher I, et al. Explicit criteria for determining inappropriate medication use in nursing home residents. Arch Intern Med. 1991;151(9):1825–32. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
