

Inflammation and airway microbiota during cystic fibrosis pulmonary exacerbations
- PMID: 23646159
- PMCID: PMC3639911
- DOI: 10.1371/journal.pone.0062917
Inflammation and airway microbiota during cystic fibrosis pulmonary exacerbations
Abstract
Background: Pulmonary exacerbations (PEx), frequently associated with airway infection and inflammation, are the leading cause of morbidity in cystic fibrosis (CF). Molecular microbiologic approaches detect complex microbiota from CF airway samples taken during PEx. The relationship between airway microbiota, inflammation, and lung function during CF PEx is not well understood.
Objective: To determine the relationships between airway microbiota, inflammation, and lung function in CF subjects treated for PEx.
Methods: Expectorated sputum and blood were collected and lung function testing performed in CF subjects during early (0-3d.) and late treatment (>7d.) for PEx. Sputum was analyzed by culture, pyrosequencing of 16S rRNA amplicons, and quantitative PCR for total and specific bacteria. Sputum IL-8 and neutrophil elastase (NE); and circulating C-reactive protein (CRP) were measured.
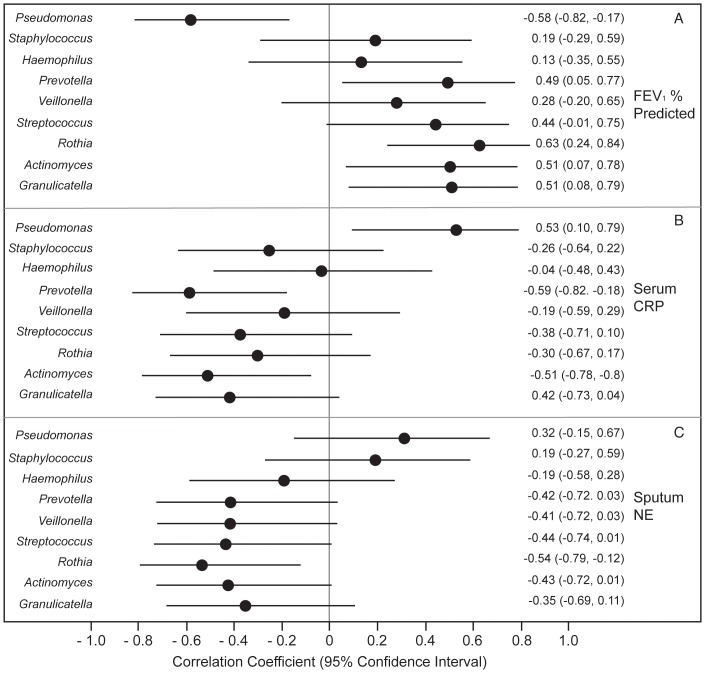
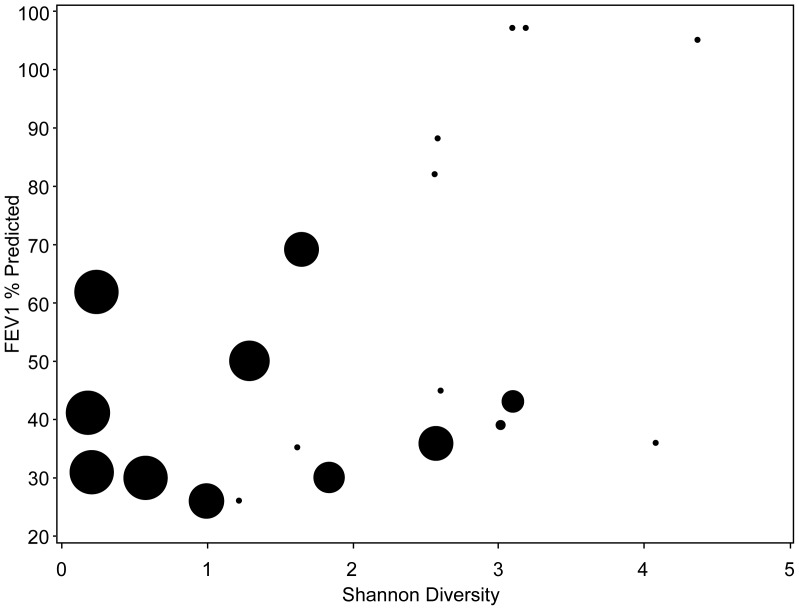
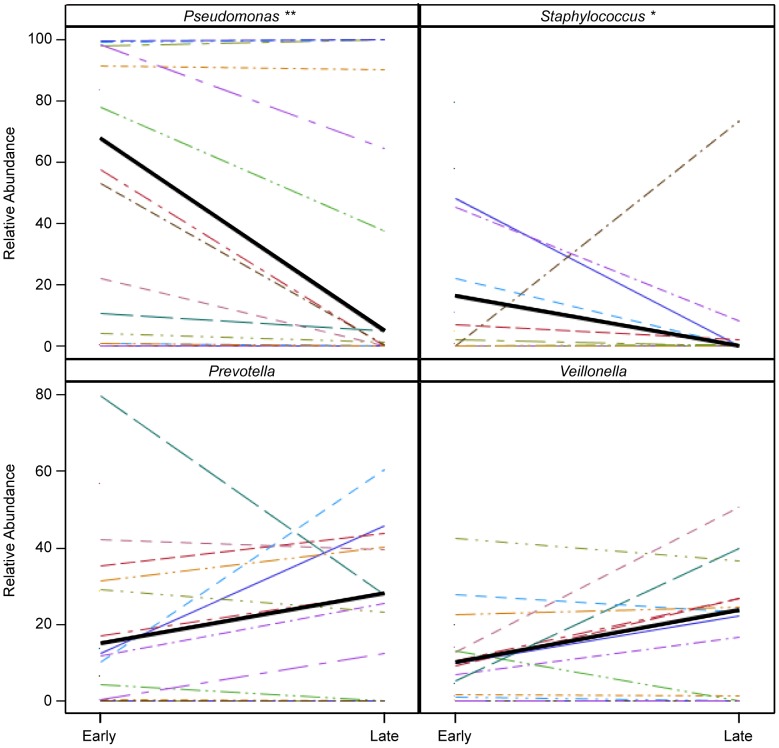
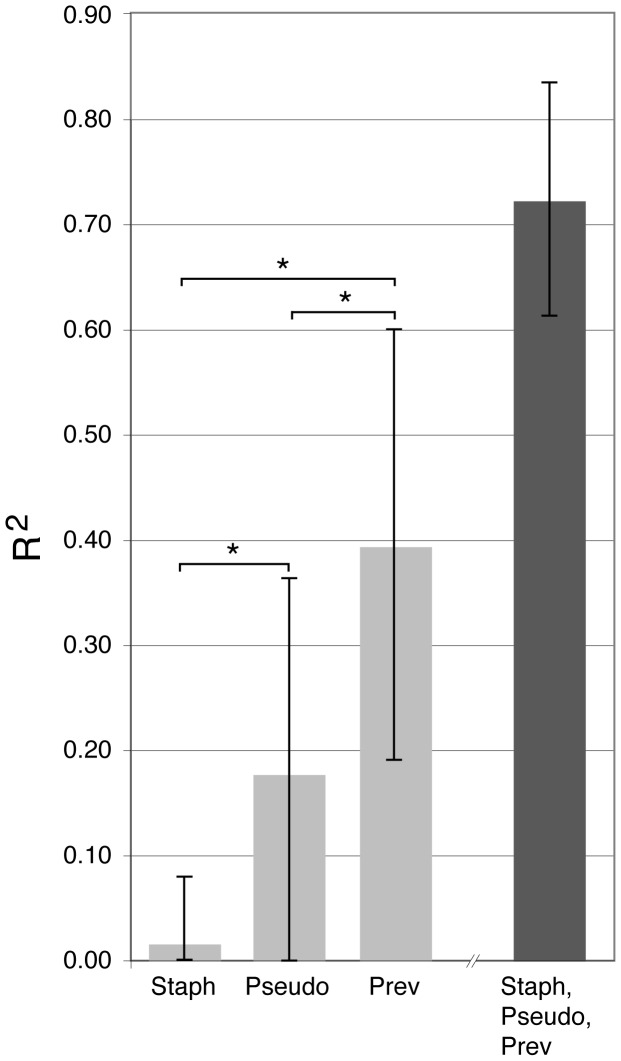
Results: Thirty-seven sputum samples were collected from 21 CF subjects. At early treatment, lower diversity was associated with high relative abundance (RA) of Pseudomonas (r = -0.67, p<0.001), decreased FEV(1%) predicted (r = 0.49, p = 0.03) and increased CRP (r = -0.58, p = 0.01). In contrast to Pseudomonas, obligate and facultative anaerobic genera were associated with less inflammation and higher FEV₁. With treatment, Pseudomonas RA and P. aeruginosa by qPCR decreased while anaerobic genera showed marked variability in response. Change in RA of Prevotella was associated with more variability in FEV₁ response to treatment than Pseudomonas or Staphylococcus.
Conclusions: Anaerobes identified from sputum by sequencing are associated with less inflammation and higher lung function compared to Pseudomonas at early exacerbation. CF PEx treatment results in variable changes of anaerobic genera suggesting the need for larger studies particularly of patients without traditional CF pathogens.
Conflict of interest statement
Figures
References
-
- Gibson RL, Burns JL, Ramsey BW (2003) Pathophysiology and management of pulmonary infections in cystic fibrosis. Am J Respir Crit Care Med 168: 918–951. - PubMed
-
- Amadori A, Antonelli A, Balteri I, Schreiber A, Bugiani M, et al. (2009) Recurrent exacerbations affect FEV(1) decline in adult patients with cystic fibrosis. Respir Med 103: 407–413. - PubMed
-
- Sanders DB, Bittner RC, Rosenfeld M, Redding GJ, Goss CH (2011) Pulmonary exacerbations are associated with subsequent FEV1 decline in both adults and children with cystic fibrosis. Pediatr Pulmonol 46: 393–400. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
