Laparoscopy-assisted gastrectomy with para-aortic lymphadenectomy after palliative chemotherapy for advanced gastric cancer with isolated para-aortic lymph node metastasis
- PMID: 23646317
- PMCID: PMC3641371
- DOI: 10.4174/jkss.2013.84.5.304
Laparoscopy-assisted gastrectomy with para-aortic lymphadenectomy after palliative chemotherapy for advanced gastric cancer with isolated para-aortic lymph node metastasis
Abstract
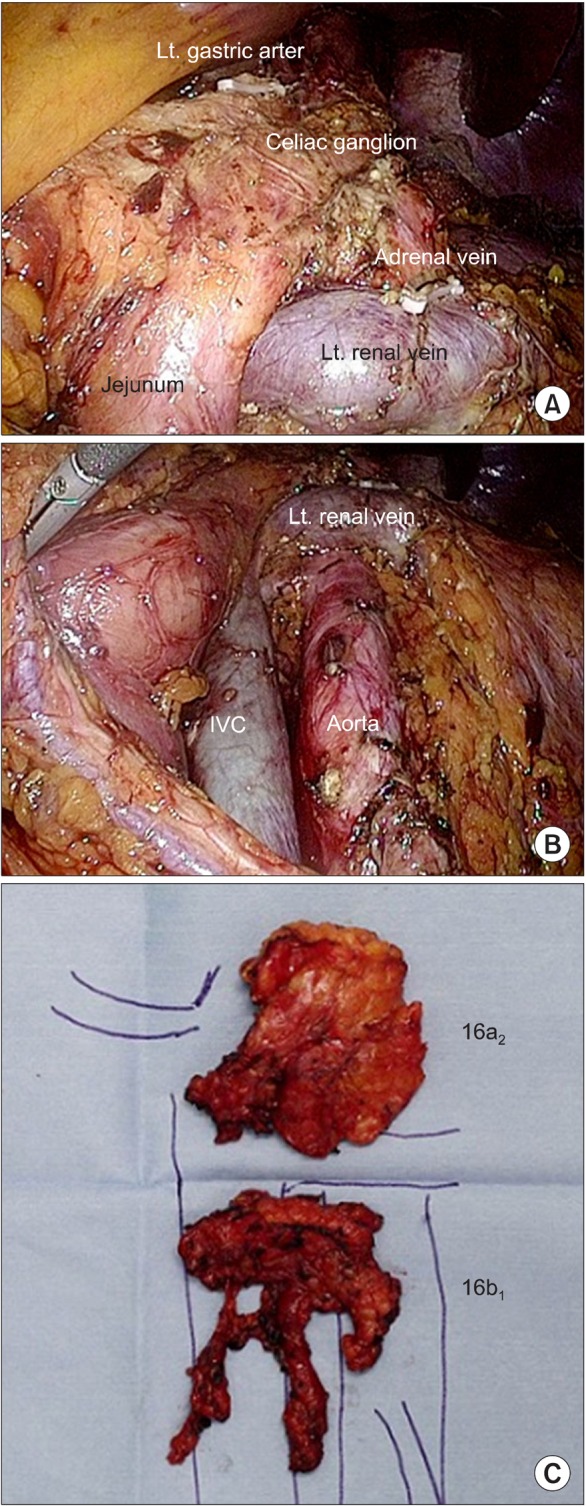
Prophylactic para-aortic lymphadenectomy is not recommended in curable advanced gastric cancer. However, there are few reports on therapeutic para-aortic lymphadenectomy after palliative chemotherapy in far advanced gastric cancer. We report three cases of laparoscopy-assisted gastrectomy with para-aortic lymphadenectomy after palliative chemotherapy for the first time in Korea. Three gastric cancer patients with isolated para-aortic lymph node (PAN) metastasis showed partial response to capecitabine-based chemotherapy, and laparoscopy-assisted gastrectomy with para-aortic lymphadenectomy was performed with curative intent. The mean total operation time was 365 minutes (range, 310 to 415 minutes), and the mean estimated blood loss was 158 mL (range, 125 to 200 mL). The mean number of retrieved PAN was 9 (range, 8 to 11), and all pathologic results showed no metastasis of para-aortic region. All patients recovered and were discharged without any significant complications.
Keywords: Gastric cancer; Laparoscopy; Para-aortic lymphadenectomy.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures

References
-
- Sasako M, Sano T, Yamamoto S, Kurokawa Y, Nashimoto A, Kurita A, et al. D2 lymphadenectomy alone or with para-aortic nodal dissection for gastric cancer. N Engl J Med. 2008;359:453–462. - PubMed
-
- Oyama K, Fushida S, Kinoshita J, Makino I, Nakamura K, Hayashi H, et al. Efficacy of pre-operative chemotherapy with docetaxel, cisplatin, and S-1 (DCS therapy) and curative resection for gastric cancer with pathologically positive para-aortic lymph nodes. J Surg Oncol. 2012;105:535–541. - PubMed
-
- Iwasaki Y, Ohashi M, Iwanaga T, Ohinata R, Takahashi K, Yamaguchi T, et al. Para-aortic lymph node dissection for far-advanced gastric cancer followed by chemotherapy. Gan To Kagaku Ryoho. 2012;39:2319–2320. - PubMed
-
- Tanaka C, Kunieda K, Kawai M, Nagao N, Nishina T, Matsuhashi N, et al. Three cases of gastric cancer with para-aortic lymph node metastases succesfully treated by S-1/CDDP combination therapy followed by curative resection. Gan To Kagaku Ryoho. 2010;37:1105–1109. - PubMed
-
- Kim H, Hyung WJ, Lim JS, Park MS, Choi JY, Chung YE, et al. Laparoscopic ultrasonography-assisted retroperitoneal lymph node sampling in patients evaluated for stomach cancer recurrence. J Ultrasound Med. 2008;27:1229–1233. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources