

Outcomes of rigid night splinting and activity modification in the treatment of cubital tunnel syndrome
- PMID: 23647638
- PMCID: PMC3989882
- DOI: 10.1016/j.jhsa.2013.02.039
Outcomes of rigid night splinting and activity modification in the treatment of cubital tunnel syndrome
Abstract
Purpose: To prospectively analyze, using validated outcome measures, symptom improvement in patients with mild to moderate cubital tunnel syndrome treated with rigid night splinting and activity modifications.
Methods: Nineteen patients (25 extremities) were enrolled prospectively between August 2009 and January 2011 following a diagnosis of idiopathic cubital tunnel syndrome. Patients were treated with activity modifications as well as a 3-month course of rigid night splinting maintaining 45° of elbow flexion. Treatment failure was defined as progression to operative management. Outcome measures included patient-reported splinting compliance as well as the Quick Disabilities of the Arm, Shoulder, and Hand questionnaire and the Short Form-12. Follow-up included a standardized physical examination. Subgroup analysis included an examination of the association between splinting success and ulnar nerve hypermobility.
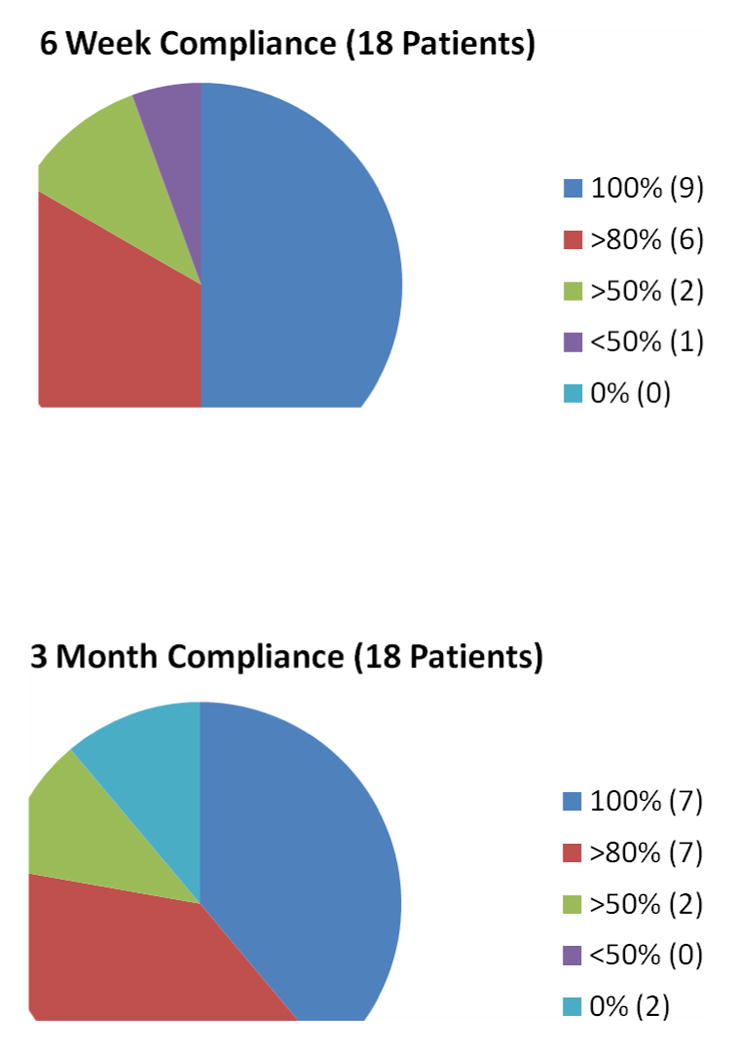
Results: Twenty-four of 25 extremities were available at mean follow-up of 2 years (range, 15-32 mo). Twenty-one of 24 (88%) extremities were successfully treated without surgery. We observed a high compliance rate with the splinting protocol during the 3-month treatment period. Quick Disabilities of the Arm, Shoulder, and Hand scores improved significantly from 29 to 11, Short Form-12 physical component summary score improved significantly from 45 to 54, and Short Form-12 mental component summary score improved significantly from 54 to 62. Average grip strength increased significantly from 32 kg to 35 kg, and ulnar nerve provocative testing resolved in 82% of patients available for follow-up examination.
Conclusions: Rigid night splinting when combined with activity modification appears to be a successful, well-tolerated, and durable treatment modality in the management of cubital tunnel syndrome. We recommend that patients presenting with mild to moderate symptoms consider initial treatment with activity modification and rigid night splinting for 3 months based on a high likelihood of avoiding surgical intervention.
Type of study/level of evidence: Therapeutic II.
Copyright © 2013 American Society for Surgery of the Hand. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Dellon AL. Review of treatment results for ulnar nerve entrapment at the elbow. J Hand Surg Am. 1989;14(4):688–700. - PubMed
-
- Bozentka DJ. Cubital tunnel syndrome pathophysiology. Clin Orthop Relat Res. 1998;(351):90–94. - PubMed
-
- Britz GW, Haynor DR, Kuntz C, et al. Ulnar nerve entrapment at the elbow: correlation of magnetic resonance imaging, clinical, electrodiagnostic, and intraoperative findings. Neurosurgery. 1996;38(3):458–465. discussion 465. - PubMed
-
- Novak CB, Lee GW, Mackinnon SE, Lay L. Provocative testing for cubital tunnel syndrome. J Hand Surg Am. 1994;19(5):817–820. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
