

Proximal superficial femoral artery occlusion, collateral vessels, and walking performance in peripheral artery disease
- PMID: 23647796
- PMCID: PMC3766720
- DOI: 10.1016/j.jcmg.2012.10.024
Proximal superficial femoral artery occlusion, collateral vessels, and walking performance in peripheral artery disease
Abstract
Objectives: We studied associations of magnetic resonance imaging (MRI)-measured superficial femoral artery (SFA) occlusions with functional performance, leg symptoms, and collateral vessel number in peripheral artery disease (PAD). We studied associations of collateral vessel number with functional performance in PAD.
Background: Associations of MRI-detected SFA occlusion and collateral vessel number with functional performance among individuals with PAD have not been reported.
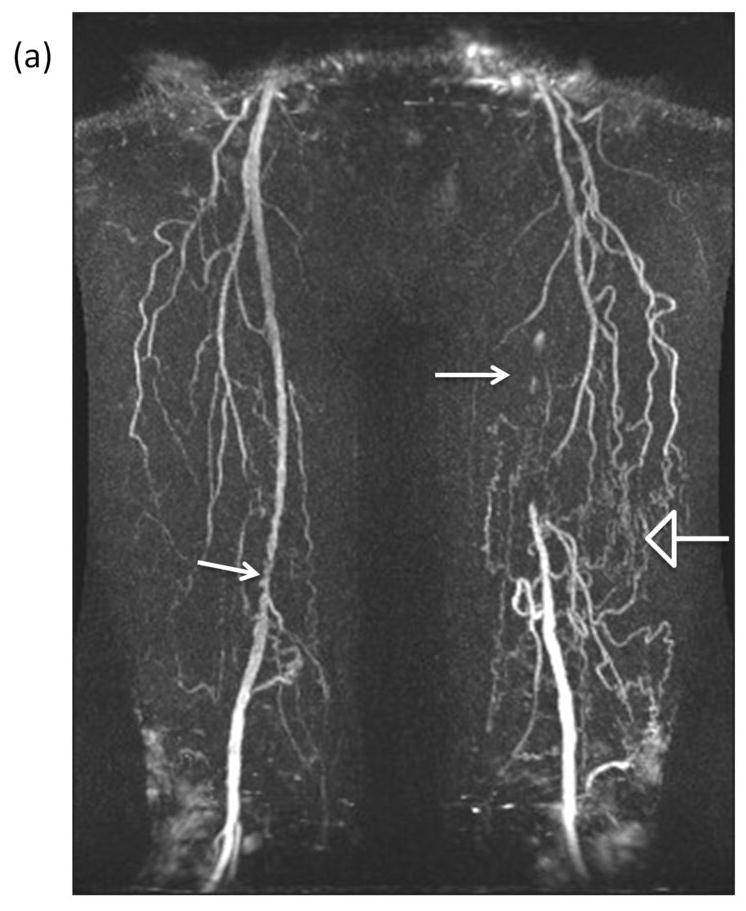
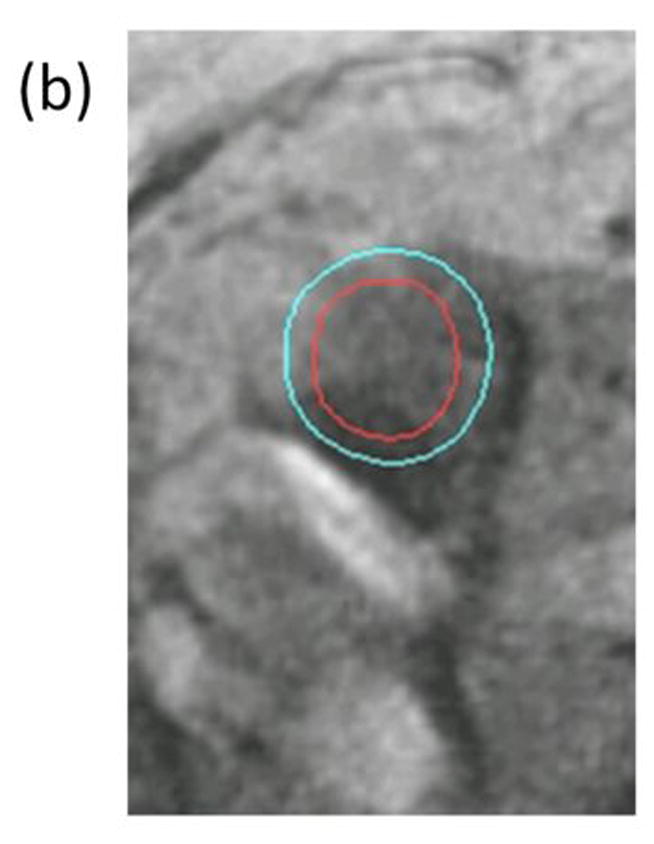
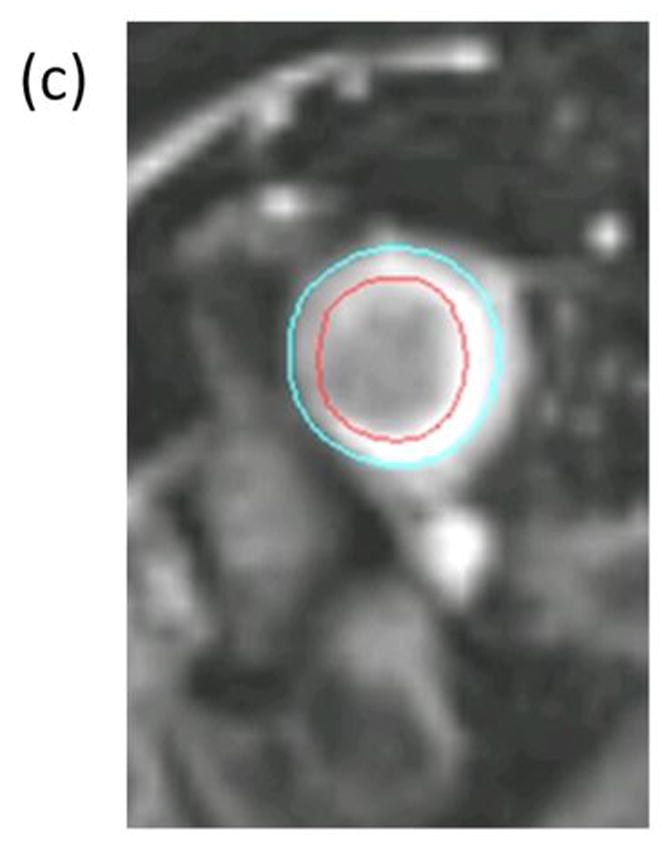
Methods: A total of 457 participants with an ankle brachial index (ABI) <1.00 had MRI measurement of the proximal SFA with 12 consecutive 2.5-μm cross-sectional images. An occluded SFA was defined as an SFA in which at least 1 segment was occluded. A nonoccluded SFA was defined as absence of any occluded slices. Collateral vessels were visualized with magnetic resonance angiography. Lower extremity functional performance was measured with the 6-min walk, 4-m walking velocity at usual and fastest pace, and the Short Physical Performance Battery (SPPB) (0 to 12 scale, 12 = best).
Results: Adjusting for age, sex, race, comorbidities, and other confounders, the presence of an SFA occlusion was associated with poorer 6-min walk performance (1,031 vs. 1,169 feet, p = 0.006), slower fast-paced walking velocity (1.15 vs. 1.22 m/s, p = 0.042), and lower SPPB score (9.07 vs. 9.75, p = 0.038) compared with the absence of an SFA occlusion. More numerous collateral vessels were associated with better 6-min walk performance (0 to 3 collaterals-1,064 feet, 4 to 7 collaterals-1,165 feet, ≥8 collaterals-1,246 feet, p trend = 0.007), faster usual-paced walking speed (0 to 3 collaterals-0.84 m/s, 4 to 7 collaterals-0.88 m/s, ≥8 collaterals-0.91 m/s, p trend = 0.029), and faster rapid-paced walking speed (0 to 3 collaterals-1.17 m/s, 4 to 7 collaterals-1.22 m/s, ≥8 collaterals-1.29 m/s, p trend = 0.002), adjusting for age, sex, race, comorbidities, ABI, and other confounders.
Conclusions: Among PAD participants, MRI-visualized occlusions in the proximal SFA are associated with poorer functional performance, whereas more numerous collaterals are associated with better functional performance. (Magnetic Resonance Imaging to Identify Characteristics of Plaque Build-Up in People With Peripheral Arterial Disease; NCT00520312).
Copyright © 2013 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Schoop W. Limb collaterals. In: Schaper W, Schaper J, editors. Collateral Circulation: Heart, Brain, Kidneys, Limbs. Kluwer Academic Publishers; Boston, MA: 1993. pp. 317–327.
-
- Prior BM, Lloyd PG, Ren J, et al. Time course of changes in collateral blood flow and isolated vessel size and gene expression after femoral artery occlusion in rats. Am J Physiol Heart Circ Physiol. 287:H2434–H2447. - PubMed
-
- Walden R, Adar R, Rubinstein ZJ, Bass A. Distribution and symmetry of arteriosclerotic lesions of the lower extremities: An arteriographic study of 200 limbs. Cardiovasc Intervent Radiol. 1985;8:108–182. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
