

Completion pneumonectomy: outcomes for benign and malignant indications
- PMID: 23647859
- PMCID: PMC3718051
- DOI: 10.1016/j.athoracsur.2013.04.014
Completion pneumonectomy: outcomes for benign and malignant indications
Abstract
Background: Past series have identified completion pneumonectomy (CP) as a high-risk operation. We evaluated factors affecting outcomes of CP with a selective approach to offering this operation.
Methods: We analyzed a prospective institutional database and abstracted information on patients undergoing pneumonectomy. Patients undergoing CP were compared with those undergoing primary pneumonectomy (PP).
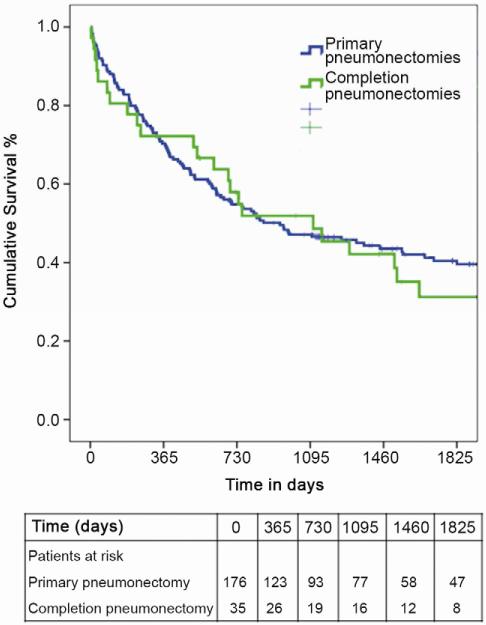
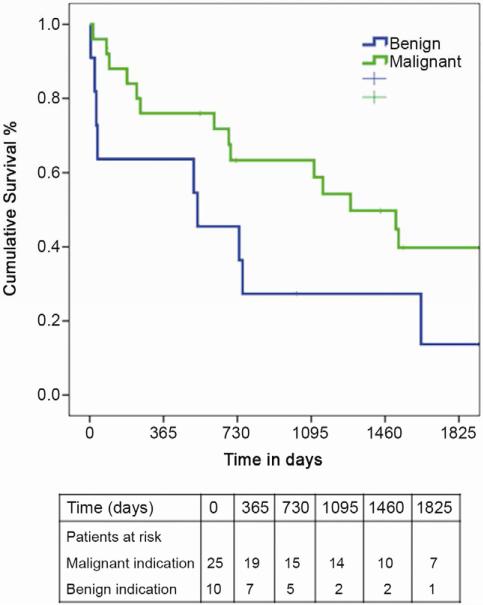
Results: Between January 2000 and February 2011, 211 patients underwent pneumonectomy, of which 35 (17%) were CPs. Ten of 35 (29%) CPs were for benign disease and 25 of 35 (71%) for cancer. Major perioperative morbidity was seen in 21 of 35 (60%) with 4 (11%) perioperative deaths. In univariate analysis, postoperative bronchopleural fistula (p = 0.05) and benign diagnosis (p = 0.07) tended to be associated with perioperative mortality. All 10 patients undergoing CP for benign disease developed a major complication compared with 11 of 25 (44%) with malignancy, p = 0.002. A bronchopleural fistula (4 of 35, 11%) was more likely to occur in patients undergoing CP shortly after the primary operation (interval between lobectomy and CP; 0.28 vs 4.5 years; p = 0.018) with a trend toward a benign indication for operation (p = 0.07). Median survival after CP for benign and malignant indications was 24.3 months and 36.5 months, respectively. Comparing CP patients to those undergoing PP (n = 176), CP patients were more likely to undergo an operation for benign disease (10 of 35, 29% vs 14 of 176, 8%, p = 0.001). Perioperative mortality for PP was 10 of 176 (5.7%), and was statistically similar to CP (11%).
Conclusions: Despite a selective approach, CP remains a morbid operation, particularly for benign indications. Rigorous preoperative optimization, ruling out contraindications to operation and attention to technical detail, are recommended.
Copyright © 2013 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Miller DL, Deschamps C, Jenkins GD, et al. Completion pneumonectomy: factors affecting operative mortality and cardiopulmonary morbidity. Ann Thorac Surg. 2002;74:876–883. discussion 883-874. - PubMed
-
- Jungraithmayr W, Hasse J, Olschewski M, Stoelben E. Indications and results of completion pneumonectomy. Eur J Cardiothorac Surg. 2004;26:189–196. - PubMed
-
- Muysoms FE, de la Riviere AB, Defauw JJ, et al. Completion pneumonectomy: analysis of operative mortality and survival. Ann Thorac Surg. 1998;66:1165–1169. - PubMed
-
- Fujimoto T, Zaboura G, Fechner S, et al. Completion pneumonectomy: current indications, complications, and results. J Thorac Cardiovasc Surg. 2001;121:484–490. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
