

Magnetic resonance imaging zygapophyseal joint space changes (gapping) in low back pain patients following spinal manipulation and side-posture positioning: a randomized controlled mechanisms trial with blinding
- PMID: 23648055
- PMCID: PMC3756802
- DOI: 10.1016/j.jmpt.2013.04.003
Magnetic resonance imaging zygapophyseal joint space changes (gapping) in low back pain patients following spinal manipulation and side-posture positioning: a randomized controlled mechanisms trial with blinding
Abstract
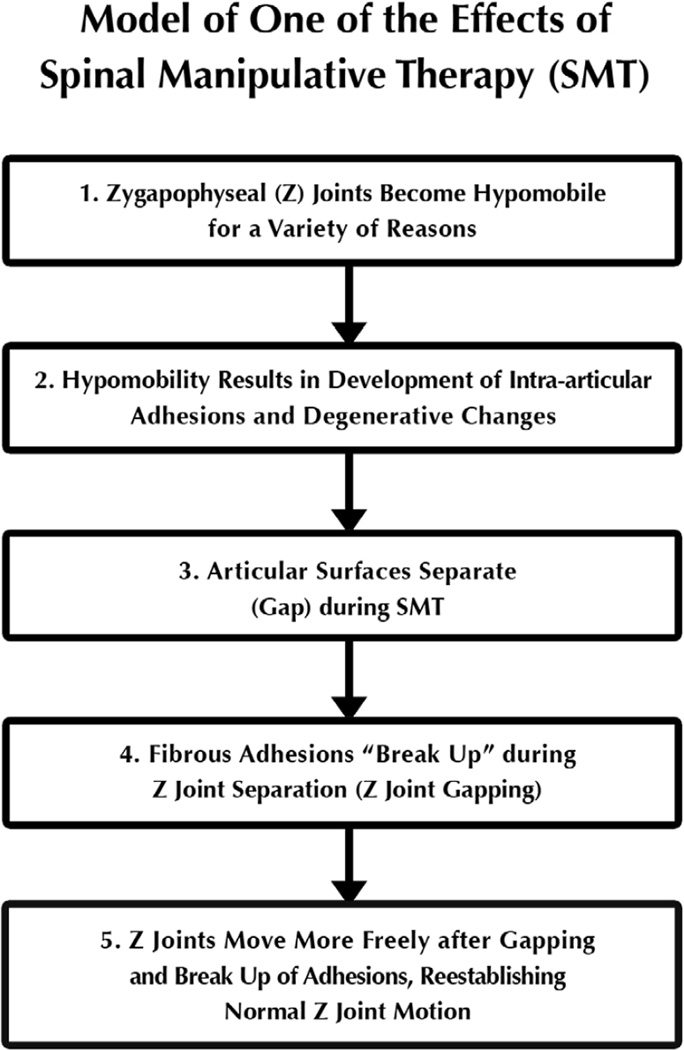
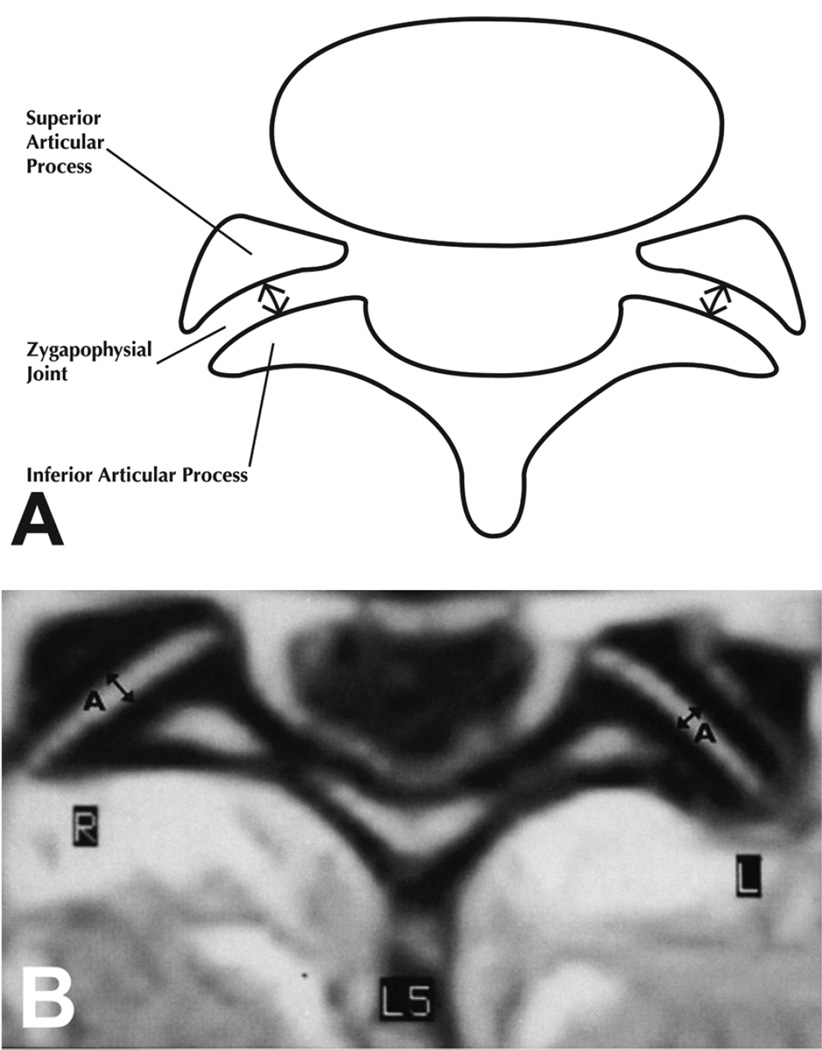
Objective: The purpose of this study was to quantify lumbar zygapophyseal (Z) joint space separation (gapping) in low back pain (LBP) subjects after spinal manipulative therapy (SMT) or side-posture positioning (SPP).
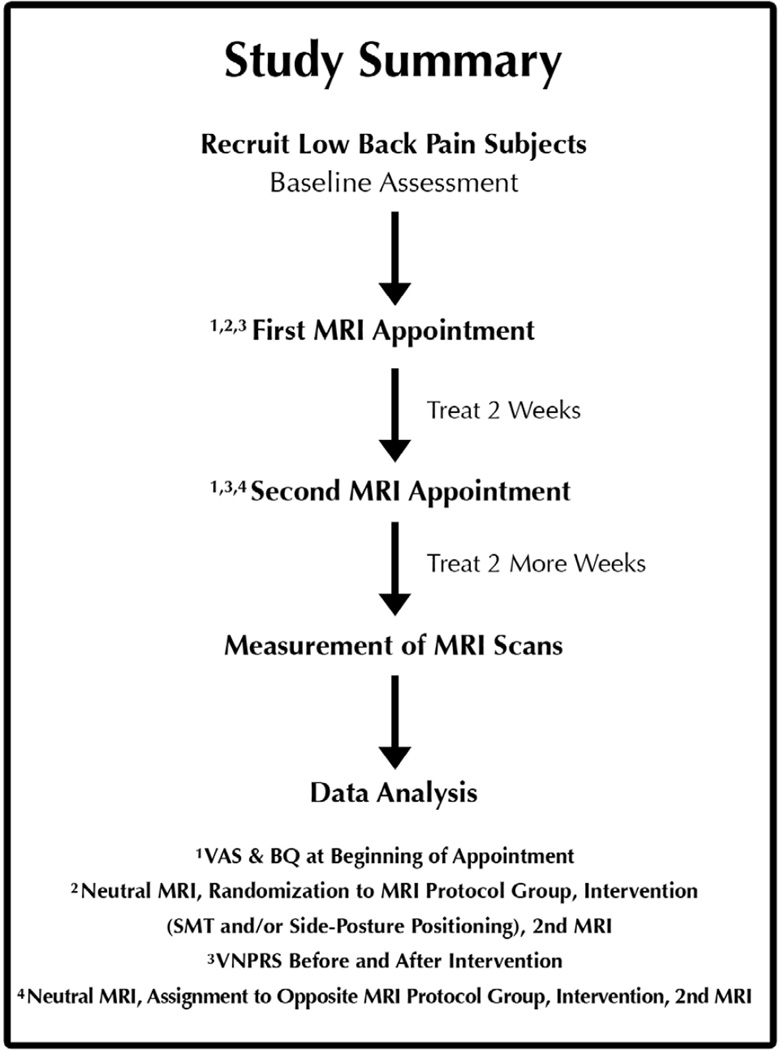
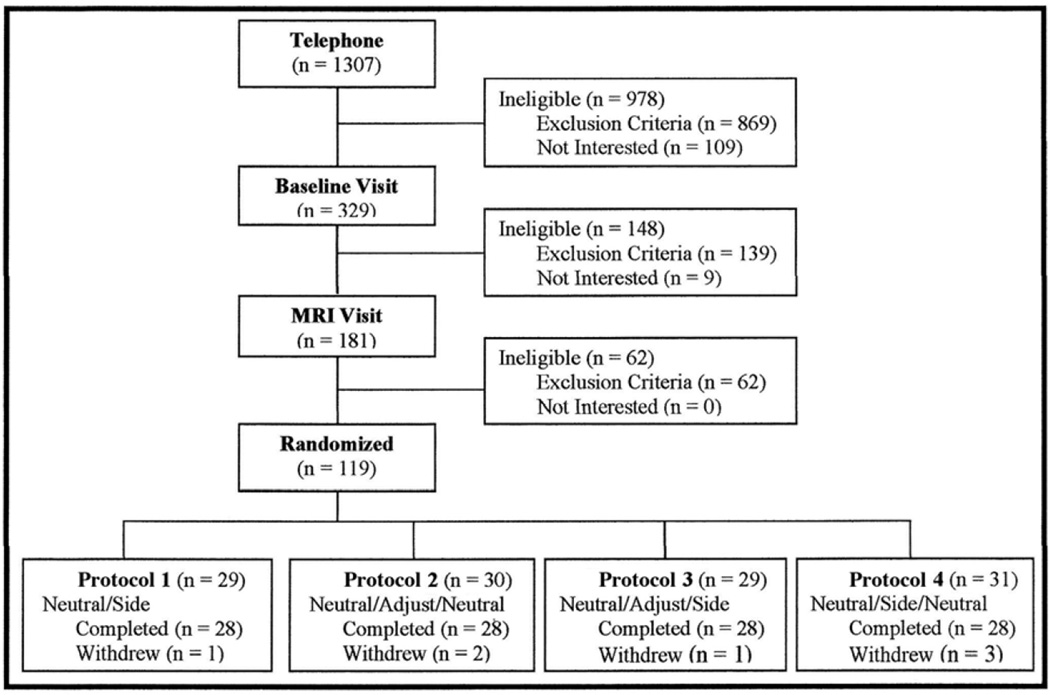
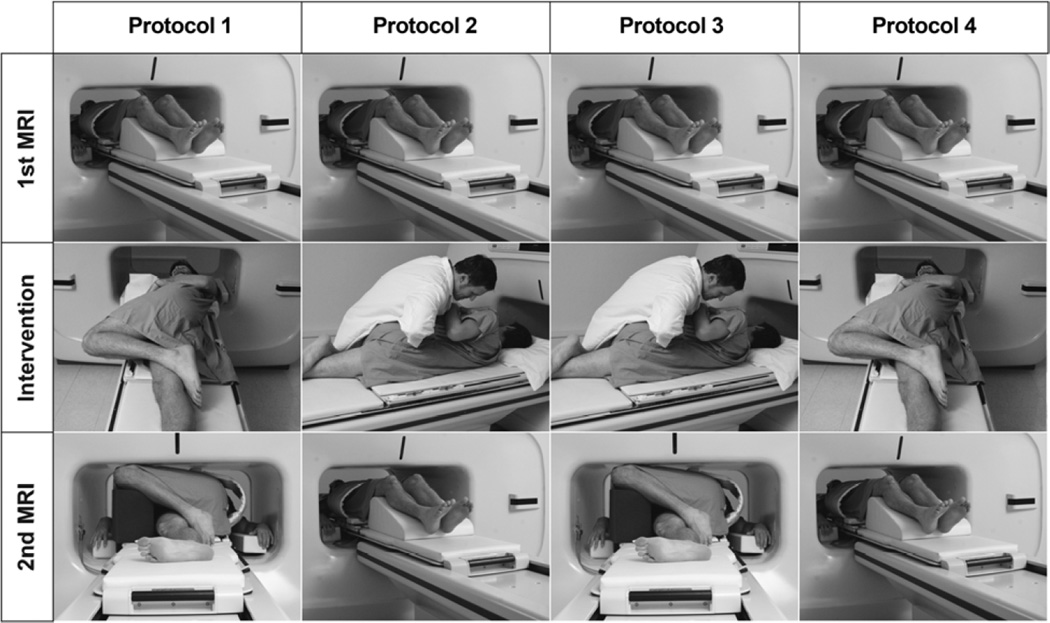
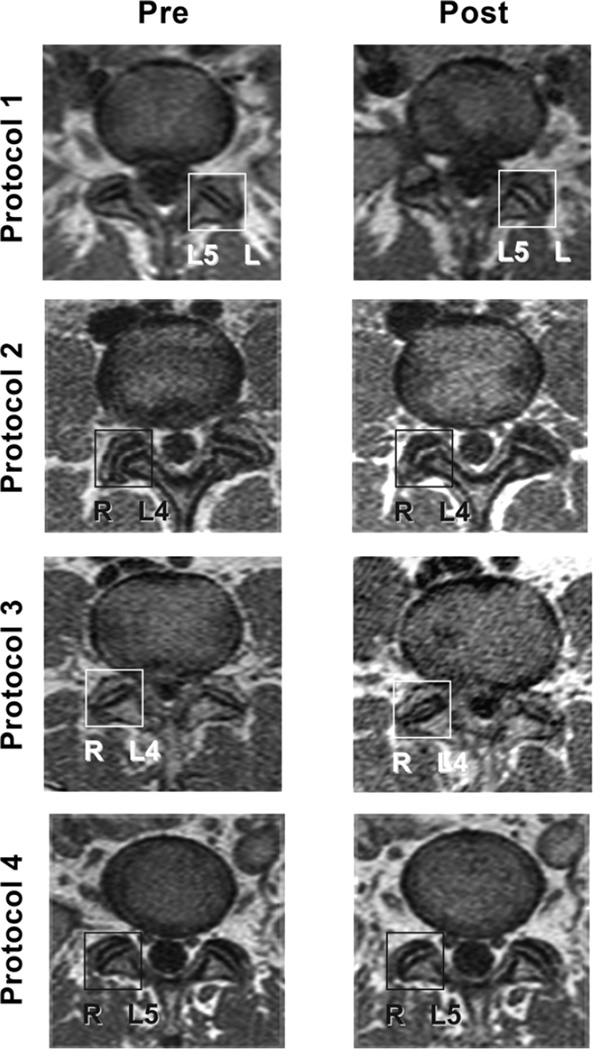
Methods: This was a controlled mechanisms trial with randomization and blinding. Acute LBP subjects (N = 112; four n = 28 magnetic resonance imaging [MRI] protocol groups) had 2 MRI appointments (initial enrollment and after 2 weeks of chiropractic treatment, receiving 2 MRI scans of the L4/L5 and L5/S1 Z joints at each MRI appointment. After the first MRI scan of each appointment, subjects were randomized (initial enrollment appointment) or assigned (after 2 weeks of chiropractic treatment appointment) into SPP (nonmanipulation), SMT (manipulation), or control MRI protocol groups. After SPP or SMT, a second MRI was taken. The central anterior-posterior joint space was measured. Difference between most painful side anterior-posterior measurements taken postintervention and preintervention was the Z joint "gapping difference." Gapping differences were compared (analysis of variance) among protocol groups. Secondary measures of pain (visual analog scale, verbal numeric pain rating scale) and function (Bournemouth questionnaire) were assessed.
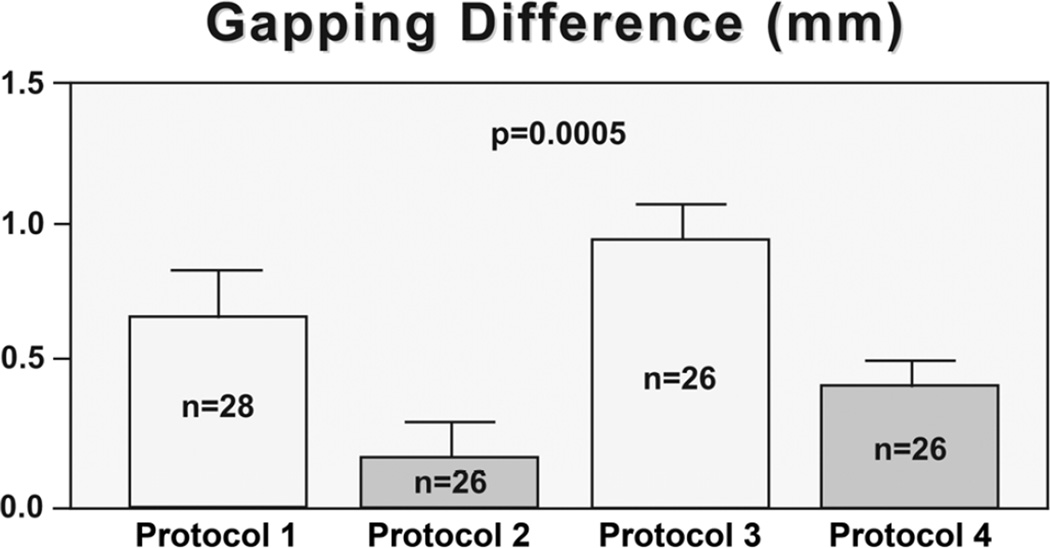
Results: Gapping differences were significant at the first (adjusted, P = .009; SPP, 0.66 ± 0.48 mm; SMT, 0.23 ± 0.86; control, 0.18 ± 0.71) and second (adjusted, P = .0005; SPP, 0.65 ± 0.92 mm; SMT, 0.89 ± 0.71; control, 0.35 ± 0.32) MRI appointments. Verbal numeric pain rating scale differences were significant at first MRI appointment (P = .04) with SMT showing the greatest improvement. Visual analog scale and Bournemouth questionnaire improved after 2 weeks of care in all groups (both P < .0001).
Conclusions: Side-posture positioning showed greatest gapping at baseline. After 2 weeks, SMT resulted in greatest gapping. Side-posture positioning appeared to have additive therapeutic benefit to SMT.
Copyright © 2013 National University of Health Sciences. Published by Mosby, Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Janse J. In: Principles and practice of chiropractic: an anthology. Hildebrandt RW, editor. Wheaton: Kjellberg & Sons; 1976. p. 326.
-
- Triano JJ. In: Interaction of spinal biomechanics and physiology. Principles and practice of chiropractic. 2nd ed. Haldeman S, editor. East Norwalk, Conn: Appleton & Lange; 1992. 1992. pp. 225–257.
-
- Evans DW. Mechanisms and effects of spinal high-velocity, low-amplitude thrust manipulation: previous theories. J Manipulative Physiol Ther. 2002;25(4):251–262. - PubMed
-
- Flynn T, Fritz J, Whitman J, Wainner R, Magel J, Rendeiro D, et al. A clinical prediction rule for classifying patients with low back pain who demonstrate short-term improvement with spinal manipulation. Spine (Phila Pa 1976) 2002;27(24):2835–43. - PubMed
-
- Fritz JM, Whitman JM, Childs JD. Lumbar spine segmental mobility assessment: an examination of validity for determining intervention strategies in patients with low back pain. Arch Phys Med Rehabil. 2005;86(9):1745–1752. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
