

Epidemiology of obstetric-related ICU admissions in Maryland: 1999-2008*
- PMID: 23648568
- PMCID: PMC3716838
- DOI: 10.1097/CCM.0b013e31828a3e24
Epidemiology of obstetric-related ICU admissions in Maryland: 1999-2008*
Abstract
Objective: To define the prevalence, indications, and temporal trends in obstetric-related ICU admissions.
Design: Descriptive analysis of utilization patterns.
Setting: All hospitals within the state of Maryland.
Patients: All antepartum, delivery, and postpartum patients who were hospitalized between 1999 and 2008.
Interventions: None.
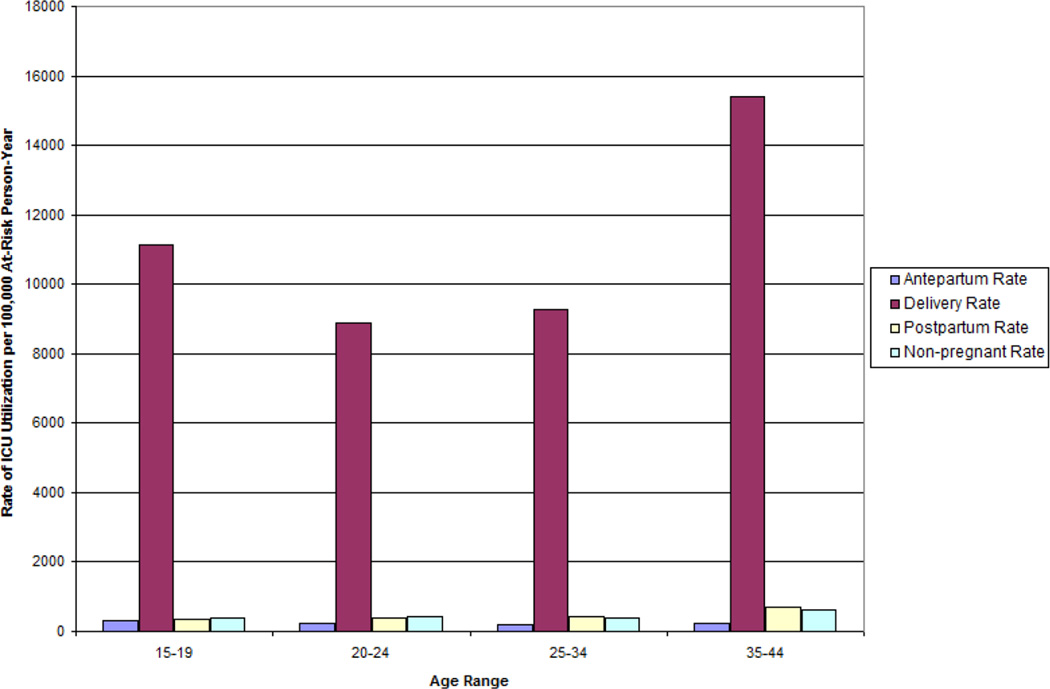
Measurements and main results: We identified 2,927 ICU admissions from 765,598 admissions for antepartum, delivery, or postpartum conditions using appropriate International Classification of Diseases, 9th Revision, Clinical Modification codes. The overall rate of ICU utilization was 419.1 per 100,000 deliveries, with rates of 162.5, 202.6, and 54.0 per 100,000 deliveries for the antepartum, delivery, and postpartum periods, respectively. The leading diagnoses associated with ICU admission were pregnancy-related hypertensive disease (present in 29.9% of admissions), hemorrhage (18.8%), cardiomyopathy or other cardiac disease (18.3%), genitourinary infection (11.5%), complications from ectopic pregnancies and abortions (10.3%), nongenitourinary infection (10.1%), sepsis (7.1%), cerebrovascular disease (5.8%), and pulmonary embolism (3.7%). We assessed for changes in the most common diagnoses in the ICU population over time and found rising rates of sepsis (10.1 per 100,000 deliveries to 16.6 per 100,000 deliveries, p = 0.003) and trauma (9.2 per 100,000 deliveries to 13.6 per 100,000 deliveries, p = 0.026) with decreasing rates of anesthetic complications (11.3 per 100,000 to 4.7 per 100,000, p = 0.006). The overall frequency of obstetric-related ICU admission and the rates for other indications remained relatively stable.
Conclusions: Between 1999 and 2008, 419.1 per 100,000 deliveries in Maryland were complicated by ICU admission. Hospitals providing obstetric services should plan for appropriate critical care management and/or transfer of women with severe morbidities during pregnancy.
Conflict of interest statement
Conflicts of interest: The authors have no financial, consultant, institutional or other relationships that might lead to bias or a conflict of interest.
Figures
Comment in
-
The risks of pregnancy in the 21st century*.Crit Care Med. 2013 Aug;41(8):2031-2. doi: 10.1097/CCM.0b013e31829a6c80. Crit Care Med. 2013. PMID: 23863234 No abstract available.
References
-
- Hogan MC, Foreman KJ, Naghavi M, Ahn SY, Wang M, Makela SM, et al. Maternal mortality for 181 countries, 1980–2008: a systematic analysis of progress towards Millennium Development Goal 5. Lancet. 2010;375(9726):1609–1623. - PubMed
-
- Geller SE, Rosenberg D, Cox SM, Brown ML, Simonson L, Driscoll CA, et al. The continuum of maternal morbidity and mortality: factors associated with severity. Am J Obstet Gynecol. 2004;191(3):939–944. - PubMed
-
- Tuncalp O, Hindin MJ, Souza JP, Chou D, Say L. The prevalence of maternal near miss: a systematic review. BJOG. 2012;119(6):653–661. - PubMed
-
- Kilpatrick SJ, Matthay MA. Obstetric patients requiring critical care. A five-year review. Chest. 1992;101(5):1407–1412. - PubMed
-
- Monaco TJ, Jr, Spielman FJ, Katz VL. Pregnant patients in the intensive care unit: a descriptive analysis. South Med J. 1993;86(4):414–417. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
