

Clinical and organizational factors in the initial evaluation of patients with lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines
- PMID: 23649435
- PMCID: PMC4694609
- DOI: 10.1378/chest.12-2352
Clinical and organizational factors in the initial evaluation of patients with lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines
Abstract
Background: This guideline is intended to provide an evidence-based approach to the initial evaluation of patients with known or suspected lung cancer. It also includes an assessment of the impact of timeliness of care and multidisciplinary teams on outcome.
Methods: The applicable current medical literature was identified by a computerized search and evaluated using standardized methods. Recommendations were framed using the approach described by the Guidelines Oversight Committee of the American College of Chest Physicians. Data sources included MEDLINE and the Cochrane Database of Systematic Reviews.
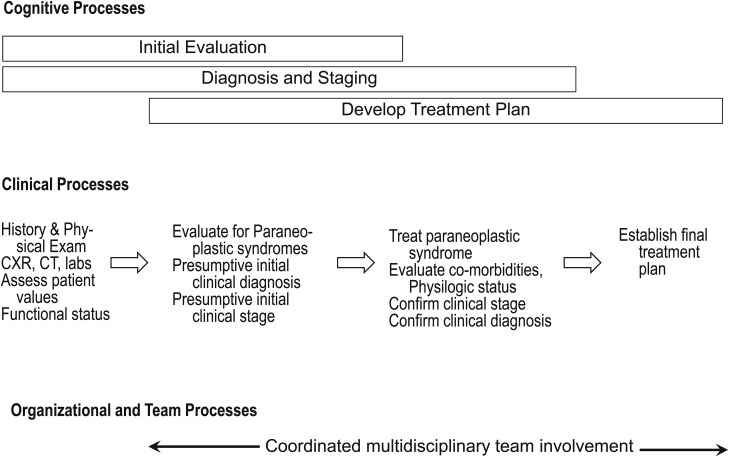
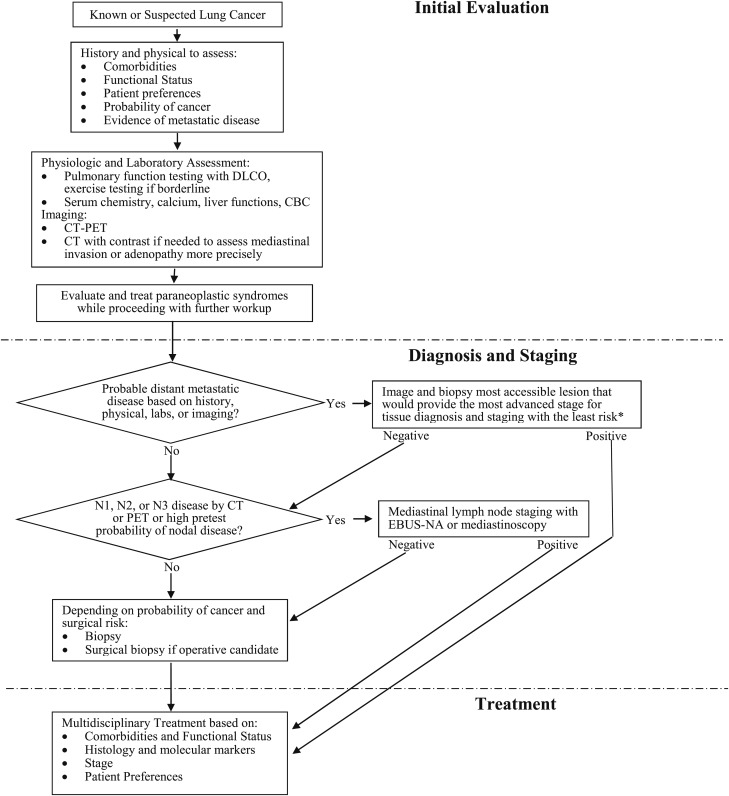
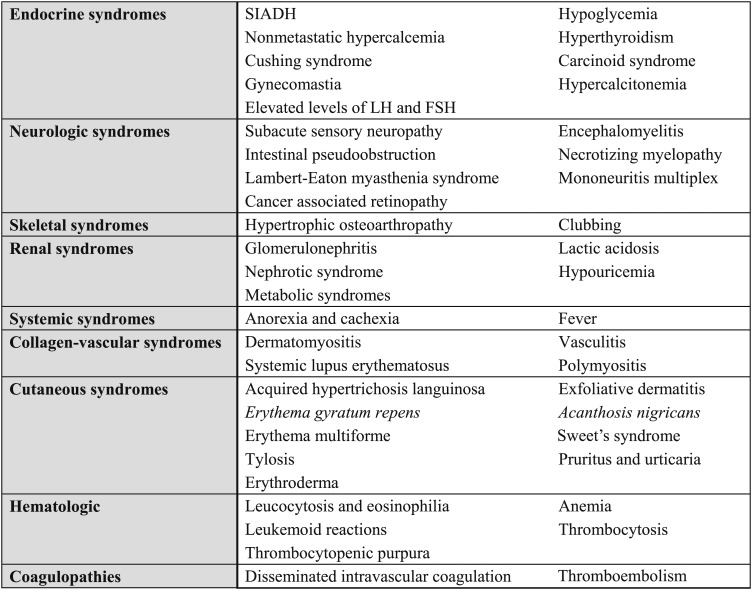
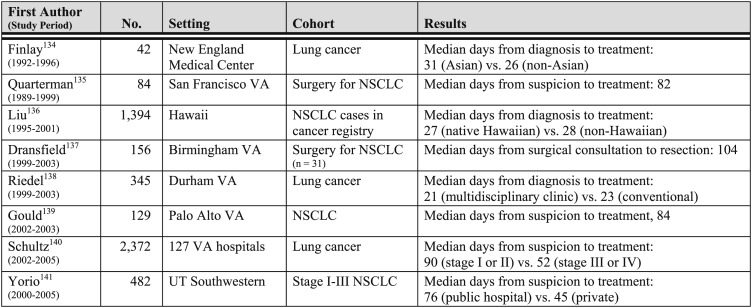
Results: Initial evaluation should include a thorough history and physical examination; CT imaging; pulmonary function tests; and hemoglobin, electrolyte, liver function, and calcium levels. Additional testing for distant metastases and paraneoplastic syndromes should be determined on the basis of these results. Paraneoplastic syndromes may have an adverse impact on cancer treatment, so they should be controlled rapidly with the goal of proceeding with definitive cancer treatment in a timely manner. Although the relationship between timeliness of care and survival is difficult to quantify, efforts to deliver timely care are reasonable and should be balanced with the need to attend to other dimensions of health-care quality (eg, safety, effectiveness, efficiency, equality, consistency with patient values and preferences). Quality care will require multiple disciplines. Although it is difficult to assess the impact, we suggest that a multidisciplinary team approach to care be used, particularly for patients requiring multimodality therapy.
Conclusions: The initial evaluation of patients with lung cancer should include a thorough history and physical examination, pulmonary function tests, CT imaging, basic laboratory tests, and selective testing for distant metastases and paraneoplastic syndromes.
Figures
References
-
- Lewis SZ, Diekemper R, Addrizzo-Harris DJ. Methodology for development of guidelines for lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143(5)(suppl):41S-50S. - PubMed
-
- Andersen H, Prakash U. Diagnosis of symptomatic lung cancer. Semin Respir Med. 1982;3(3):165-175.
-
- Grippi MA. Clinical aspects of lung cancer. Semin Roentgenol. 1990;25(1):12-24. - PubMed
-
- Hyde L, Hyde CI. Clinical manifestations of lung cancer. Chest. 1974;65(3):299-306. - PubMed
-
- Cromartie RS, III, Parker EF, May JE, Metcalf JS, Bartles DM. Carcinoma of the lung: a clinical review. Ann Thorac Surg. 1980;30(1):30-35. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
