

Screening for lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines
- PMID: 23649455
- PMCID: PMC3749713
- DOI: 10.1378/chest.12-2350
Screening for lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines
Abstract
Background: Lung cancer is by far the major cause of cancer deaths largely because in the majority of patients it is at an advanced stage at the time it is discovered, when curative treatment is no longer feasible. This article examines the data regarding the ability of screening to decrease the number of lung cancer deaths.
Methods: A systematic review was conducted of controlled studies that address the effectiveness of methods of screening for lung cancer.
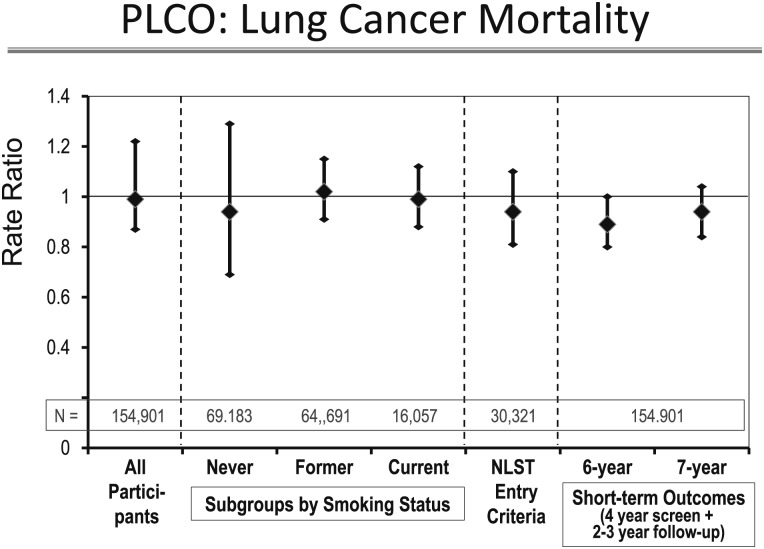
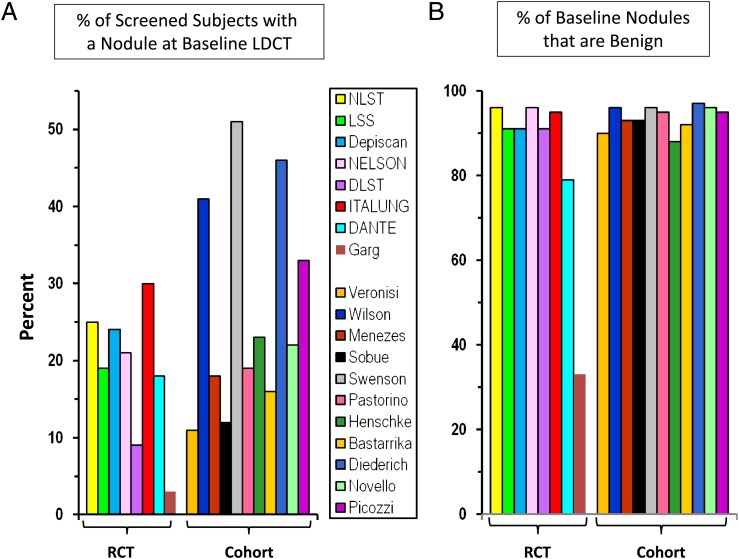
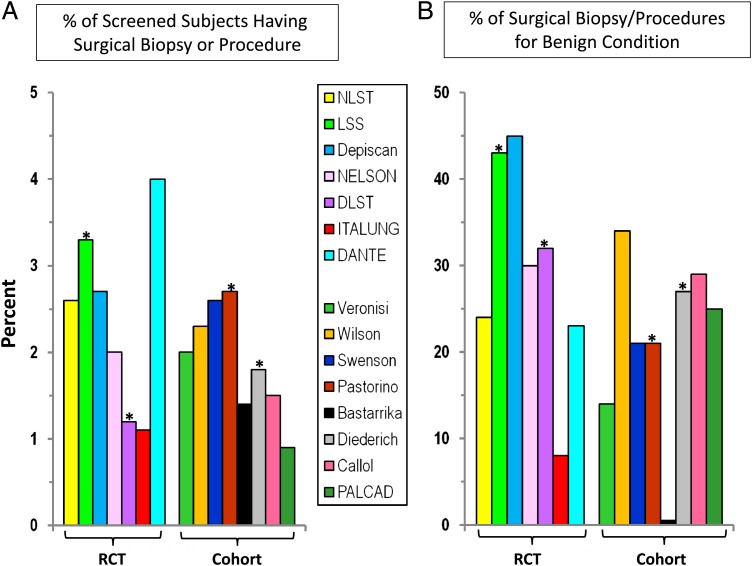
Results: Several large randomized controlled trials (RCTs), including a recent one, have demonstrated that screening for lung cancer using a chest radiograph does not reduce the number of deaths from lung cancer. One large RCT involving low-dose CT (LDCT) screening demonstrated a significant reduction in lung cancer deaths, with few harms to individuals at elevated risk when done in the context of a structured program of selection, screening, evaluation, and management of the relatively high number of benign abnormalities. Whether other RCTs involving LDCT screening are consistent is unclear because data are limited or not yet mature.
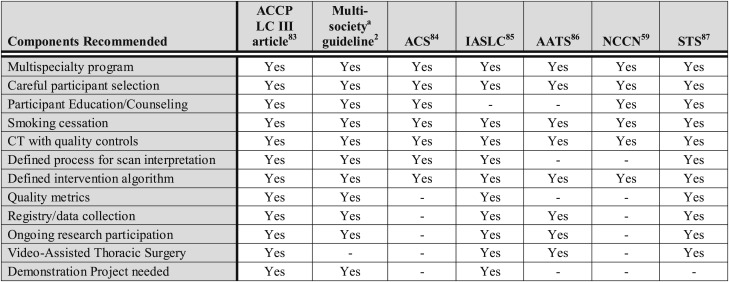
Conclusions: Screening is a complex interplay of selection (a population with sufficient risk and few serious comorbidities), the value of the screening test, the interval between screening tests, the availability of effective treatment, the risk of complications or harms as a result of screening, and the degree with which the screened individuals comply with screening and treatment recommendations. Screening with LDCT of appropriate individuals in the context of a structured process is associated with a significant reduction in the number of lung cancer deaths in the screened population. Given the complex interplay of factors inherent in screening, many questions remain on how to effectively implement screening on a broader scale.
Figures
Comment in
-
Targeted CT image screening and its effect on lung cancer detection rate.Chest. 2013 Oct;144(4):1419-1420. doi: 10.1378/chest.13-1321. Chest. 2013. PMID: 24081361 No abstract available.
-
Response.Chest. 2013 Oct;144(4):1420-1421. doi: 10.1378/chest.13-1350. Chest. 2013. PMID: 24081362 No abstract available.
-
Lung cancer screening.Chest. 2013 Nov;144(5):1737. doi: 10.1378/chest.13-1539. Chest. 2013. PMID: 24189878 No abstract available.
-
Response.Chest. 2013 Nov;144(5):1737-1738. doi: 10.1378/chest.13-1736. Chest. 2013. PMID: 24189879 No abstract available.
References
-
- Lewis SZ, Diekemper R, Addrizzo-Harris DJ. Methodology for development of guidelines for lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143(5)(suppl):41S-50S - PubMed
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62(1):10-29 - PubMed
-
- Wegwarth O, Schwartz LM, Woloshin S, Gaissmaier W, Gigerenzer G. Do physicians understand cancer screening statistics? A national survey of primary care physicians in the United States. Ann Intern Med. 2012;156(5):340-349 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
