

Community-partnered cluster-randomized comparative effectiveness trial of community engagement and planning or resources for services to address depression disparities
- PMID: 23649787
- PMCID: PMC3785665
- DOI: 10.1007/s11606-013-2484-3
Community-partnered cluster-randomized comparative effectiveness trial of community engagement and planning or resources for services to address depression disparities
Erratum in
- J Gen Intern Med. 2013 Nov;28(11):1534
Abstract
Background: Depression contributes to disability and there are ethnic/racial disparities in access and outcomes of care. Quality improvement (QI) programs for depression in primary care improve outcomes relative to usual care, but health, social and other community-based service sectors also support clients in under-resourced communities. Little is known about effects on client outcomes of strategies to implement depression QI across diverse sectors.
Objective: To compare the effectiveness of Community Engagement and Planning (CEP) and Resources for Services (RS) to implement depression QI on clients' mental health-related quality of life (HRQL) and services use.
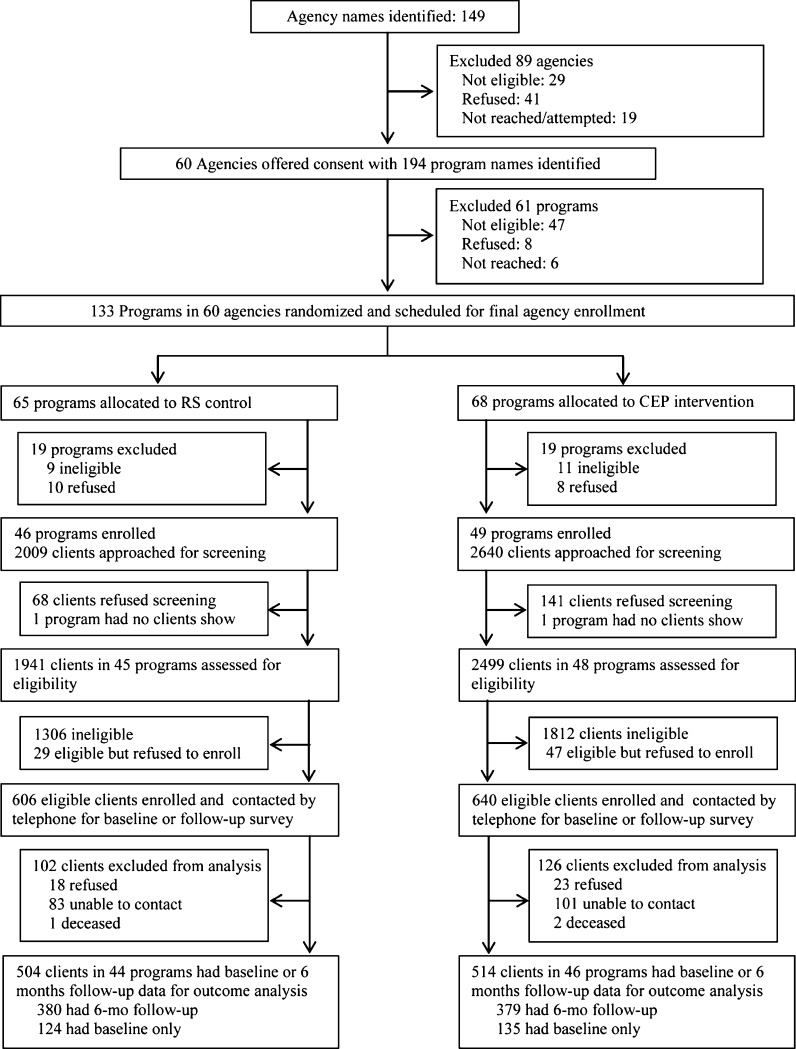
Design: Matched programs from health, social and other service sectors were randomized to community engagement and planning (promoting inter-agency collaboration) or resources for services (individual program technical assistance plus outreach) to implement depression QI toolkits in Hollywood-Metro and South Los Angeles.
Participants: From 93 randomized programs, 4,440 clients were screened and of 1,322 depressed by the 8-item Patient Health Questionnaire (PHQ-8) and providing contact information, 1,246 enrolled and 1,018 in 90 programs completed baseline or 6-month follow-up.
Measures: Self-reported mental HRQL and probable depression (primary), physical activity, employment, homelessness risk factors (secondary) and services use.
Results: CEP was more effective than RS at improving mental HRQL, increasing physical activity and reducing homelessness risk factors, rate of behavioral health hospitalization and medication visits among specialty care users (i.e. psychiatrists, mental health providers) while increasing depression visits among users of primary care/public health for depression and users of faith-based and park programs (each p < 0.05). Employment, use of antidepressants, and total contacts were not significantly affected (each p > 0.05).
Conclusion: Community engagement to build a collaborative approach to implementing depression QI across diverse programs was more effective than resources for services for individual programs in improving mental HRQL, physical activity and homelessness risk factors, and shifted utilization away from hospitalizations and specialty medication visits toward primary care and other sectors, offering an expanded health-home model to address multiple disparities for depressed safety-net clients.
Figures
Comment in
-
Depression research in under-resourced populations: an academic-community partnership.J Gen Intern Med. 2013 Oct;28(10):1255-7. doi: 10.1007/s11606-013-2495-0. J Gen Intern Med. 2013. PMID: 23677462 Free PMC article. No abstract available.
-
Applying Community-Partnered Participatory Research Approaches to Develop COVID-19 Solutions.Ethn Dis. 2020 Jul 9;30(3):433-436. doi: 10.18865/ed.30.3.433. eCollection 2020 Summer. Ethn Dis. 2020. PMID: 32742147 Free PMC article. No abstract available.
References
-
- Williams DR, Gonzalez HM, Neighbors H, Nesse R, Abelson JM, Sweetman J, et al. Prevalence and distribution of major depressive disorder in African Americans, Caribbean blacks, and non-Hispanic whites: results from the National Survey of American Life. Arch Gen Psychiatry. 2007;64(3):305–15. doi: 10.1001/archpsyc.64.3.305. - DOI - PubMed
-
- Miranda J, Duan N, Sherbourne C, Schoenbaum M, Lagomasino I, Jackson-Triche M, et al. Improving care for minorities: can quality improvement interventions improve care and outcomes for depressed minorities? Results of a controlled randomized trial. Health Serv Res. 2003;38(2):613–30. doi: 10.1111/1475-6773.00136. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
