

Ovarian cancer incidence trends in relation to changing patterns of menopausal hormone therapy use in the United States
- PMID: 23650423
- PMCID: PMC3731982
- DOI: 10.1200/JCO.2012.45.5758
Ovarian cancer incidence trends in relation to changing patterns of menopausal hormone therapy use in the United States
Abstract
Purpose: After a report from the Women's Health Initiative (WHI) in 2002, a precipitous decline in menopausal hormonal therapy (MHT) use in the United States was linked to a decline in breast cancer incidence rates. Given that MHT use is also associated with increased ovarian cancer risk, we tested whether ovarian cancer incidence rates changed after 2002.
Methods: Using the North American Association of Central Cancer Registries database (1995 to 2008; N = 171,142 incident ovarian cancers), we applied standard analytic approaches and age-period-cohort (APC) models to estimate ovarian cancer incidence rate changes before (1995 to 2002) and after (2003 to 2008) the WHI report.
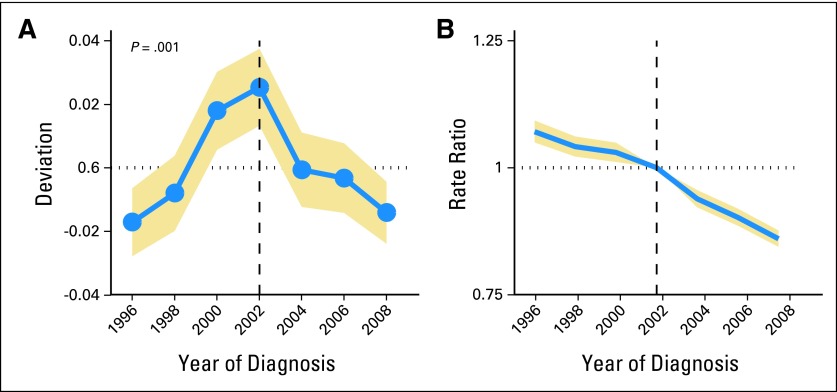
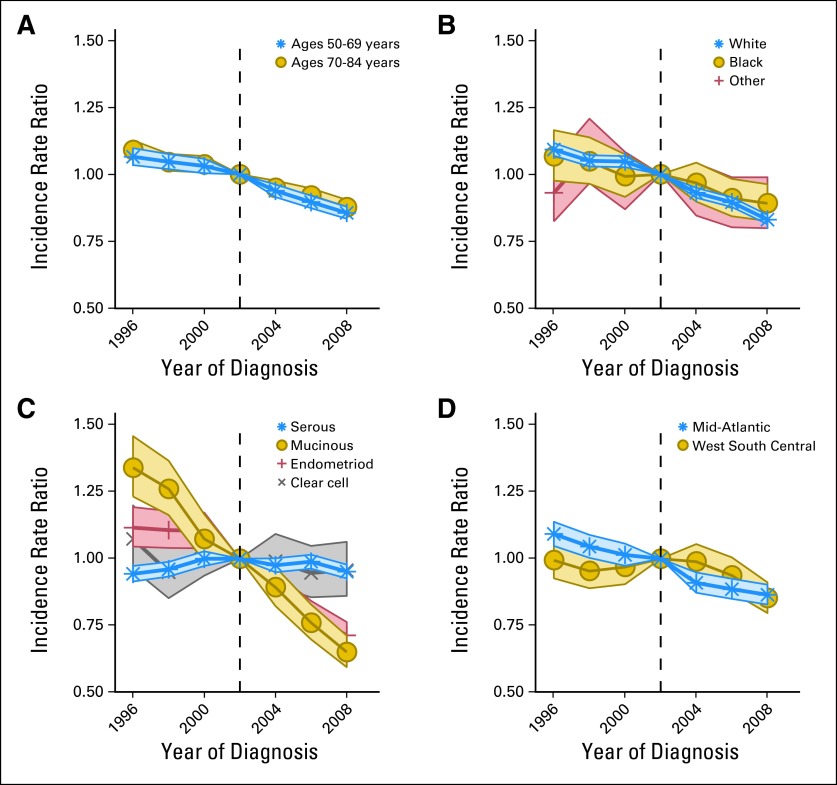
Results: Among women age ≥ 50 years, age-standardized ovarian cancer incidence declined by 0.8% per year (95% CI, -1.8% to -0.5% per year) before the WHI announcement; after the WHI report, the rate declined by 2.4% per year (95% CI, -2.5% to -2.2% per year). APC models confirmed an accelerated decline in ovarian cancer incidence after the WHI report, adjusted for age and birth cohort effects. This sudden change was notable among women most likely to have used MHT (ie, women age 50 to 69 years, white women, and residents of regions with highest MHT prescription frequency). The largest changes were found for the endometrioid histologic subtype.
Conclusion: After a marked reduction in MHT use around 2002, ovarian cancer incidence rates demonstrated an accelerated decline, with the largest changes for endometrioid carcinomas. This strong temporal association, although not proving a causal role of hormones in ovarian carcinogenesis, suggests that future analytic research supporting cancer control efforts should clarify the role of hormonal exposures on the development and behavior of subtypes of ovarian cancer.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures

References
-
- American Cancer Society. Atlanta, GA: American Cancer Society; 2012. Cancer Facts & Figures.
-
- Weiss NS, Szekely DR, Austin DF. Increasing incidence of endometrial cancer in the United States. N Engl J Med. 1976;294:1259–1262. - PubMed
-
- Rossouw JE, Anderson GL, Prentice RL, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: Principal results from the Women's Health Initiative randomized controlled trial. JAMA. 2002;288:321–333. - PubMed
-
- Buist DS, Newton KM, Miglioretti DL, et al. Hormone therapy prescribing patterns in the United States. Obstet Gynecol. 2004;104:1042–1050. - PubMed
-
- Hersh AL, Stefanick ML, Stafford RS. National use of postmenopausal hormone therapy: Annual trends and response to recent evidence. JAMA. 2004;291:47–53. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
