

Assessment of a pharmacogenomic marker panel in a polypharmacy population identified from electronic medical records
- PMID: 23651022
- PMCID: PMC3725600
- DOI: 10.2217/pgs.13.64
Assessment of a pharmacogenomic marker panel in a polypharmacy population identified from electronic medical records
Abstract
Background: The ADME Core Panel assays 184 variants across 34 pharmacogenes, many of which are difficult to accurately genotype with standard multiplexing methods.
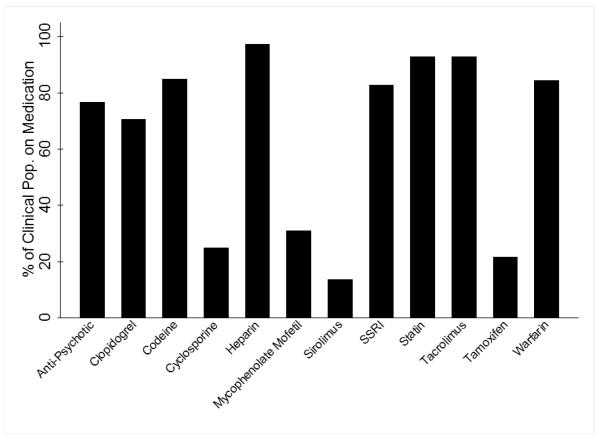
Methods: We genotyped 326 frequently medicated individuals of European descent in Vanderbilt's biorepository linked to de-identified electronic medical records, BioVU, on the ADME Core Panel to assess quality and performance of the assay. We compared quality control metrics and determined the extent of direct and indirect marker overlap between the ADME Core Panel and the Illumina Omni1-Quad.
Results: We found the quality of the ADME Core Panel data to be high, with exceptions in select copy number variants and markers in certain genes (notably CYP2D6). Most of the common variants on the ADME panel are genotyped by the Omni1, but absent rare variants and copy number variants could not be accurately tagged by single markers.
Conclusion: Our frequently medicated study population did not convincingly differ in allele frequency from reference populations, suggesting that heterogeneous clinical samples (with respect to medications) have similar allele frequency distributions in pharmacogenetics genes compared with reference populations.
Figures
References
-
-
Peters EJ, McLeod HL. Ability of whole-genome SNP arrays to capture ’must have’ pharmacogenomic variants. Pharmacogenomics. 2008;9(11):1573–1577.** Discusses the Pharmacogenetics Research Network’s very important pharmacogenes list and their coverage of genome-wide platforms
-
-
- Sim SC, Ingelman-Sundberg M. Pharmacogenomic biomarkers: new tools in current and future drug therapy. Trends Pharmacol.Sci. 2011;32(2):72–81. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources