

Prostate rotation detected from implanted markers can affect dose coverage and cannot be simply dismissed
- PMID: 23652257
- PMCID: PMC5714427
- DOI: 10.1120/jacmp.v14i3.4262
Prostate rotation detected from implanted markers can affect dose coverage and cannot be simply dismissed
Abstract
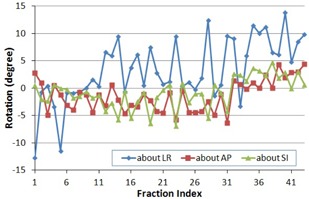
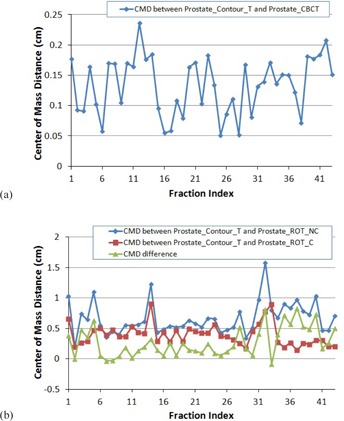
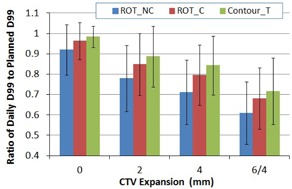
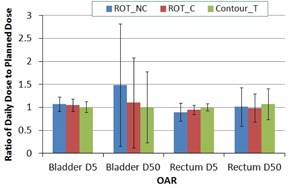
With implanted markers, daily prostate displacements can be automatically detected with six degrees of freedom. The reported magnitudes of the rotations, however, are often greater than the typical range of a six-degree treatment couch. The purpose of this study is to quantify geometric and dosimetric effects if the prostate rotations are not corrected (ROT_NC) and if they can be compensated with translational shifts (ROT_C). Forty-three kilovoltage cone-beam CTs (KV-CBCT) with implanted markers from five patients were available for this retrospective study. On each KV-CBCT, the prostate, bladder, and rectum were manually contoured by a physician. The prostate contours from the planning CT and CBCT were aligned manually to achieve the best overlaps. This contour registration served as the benchmark method for comparison with two marker registration methods: (a) using six degrees of freedom, but rotations were not corrected (ROT_NC); and (b) using three degrees of freedom while compensating rotations into the translational shifts (ROT_C). The center of mass distance (CMD) and overlap index (OI) were used to evaluate these two methods. The dosimetric effects were also analyzed by comparing the dose coverage of the prostate clinical target volume (CTV) in relation to the planning margins. According to our analysis, the detected rotations dominated in the left-right axis with systematic and random components of 4.6° and 4.1°, respectively. When the rotation angles were greater than 10°, the differences in CMD between the two registrations were greater than 5 mm in 85.7% of these fractions; when the rotation angles were greater than 6°, the differences of CMD were greater than 4 mm in 61.1% of these fractions. With 6 mm/4 mm posterior planning margins, the average difference between the dose to 99% (D99) of the prostate in CBCTs and the planning D99 of the prostate was -8.0 ± 12.3% for the ROT_NC registration, and -3.6 ± 9.0% for the ROT_C registration (p = 0.01). When the planning margin decreased to 4 mm/2 mm posterior, the average difference in D99 of the prostate was -22.0 ± 16.2% and -15.1 ± 15.2% for the ROT_NC and ROT_C methods, respectively (p < 0.05). In conclusion, prostate rotation cannot be simply dismissed, and the impact of the rotational errors depends on the distance between the isocenter and the centroid of implanted markers and the rotation angle.
Figures


References
-
- Langen KM and Jones DT. Organ motion and its management. Int J Radiat Oncol Biol Phys. 2001;50(1):265–78. - PubMed
-
- Byrne TE. A review of prostate motion with considerations for the treatment of prostate cancer. Med Dosim. 2005;30(3):155–61. - PubMed
-
- van Herk M, Bruce A, Kroes AP, Shouman T, Touw A, Lebesque JV. Quantification of organ motion during conformal radiotherapy of the prostate by three dimensional image registration. Int J Radiat Oncol Biol Phys. 1995;33(5):1311–20. - PubMed
-
- Hanley J, Lumley MA, Mageras GS, et al. Measurement of patient positioning errors in three‐dimensional conformal radiotherapy of the prostate. Int J Radiat Oncol Biol Phys. 1997;37(2):435–44. - PubMed
-
- Remeijer P, Geerlof E, Ploeger L, Gilhuijs K, van Herk M, Lebesque J V. 3‐D portal image analysis in clinical practice: an evaluation of 2‐D and 3‐D analysis techniques as applied to 30 prostate cancer patients. Int J Radiat Oncol Biol Phys. 2000;46(5):1281–90. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
