

Volumetric-modulated arc therapy for the treatment of a large planning target volume in thoracic esophageal cancer
- PMID: 23652258
- PMCID: PMC5714417
- DOI: 10.1120/jacmp.v14i3.4269
Volumetric-modulated arc therapy for the treatment of a large planning target volume in thoracic esophageal cancer
Abstract
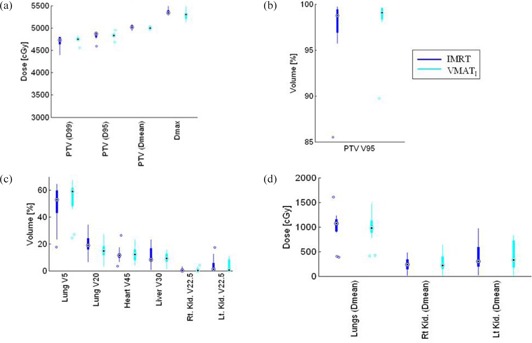
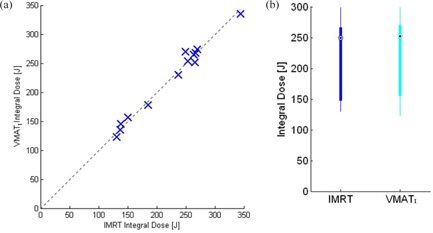
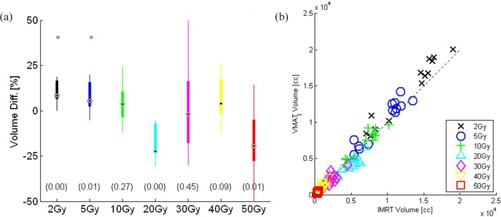
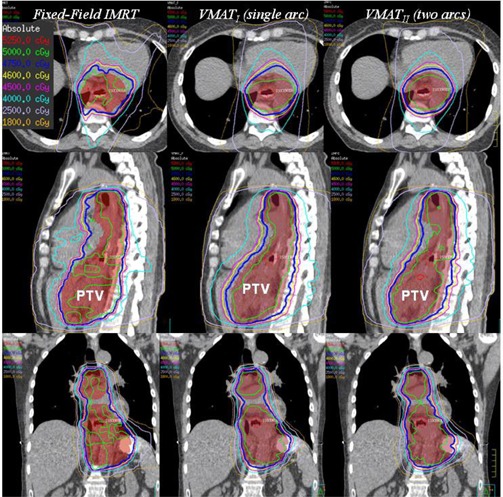
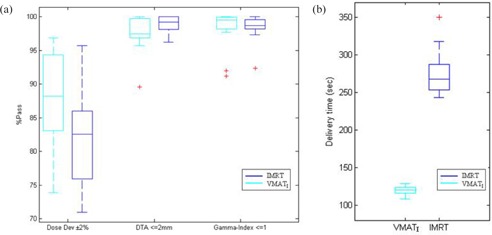
Recently, volumetric-modulated arc therapy (VMAT) has demonstrated the ability to deliver radiation dose precisely and accurately with a shorter delivery time compared to conventional intensity-modulated fixed-field treatment (IMRT). We applied the hypothesis of VMAT technique for the treatment of thoracic esophageal carcinoma to determine superior or equivalent conformal dose coverage for a large thoracic esophageal planning target volume (PTV) with superior or equivalent sparing of organs-at-risk (OARs) doses, and reduce delivery time and monitor units (MUs), in comparison with conventional fixed-field IMRT plans. We also analyzed and compared some other important metrics of treatment planning and treatment delivery for both IMRT and VMAT techniques. These metrics include: 1) the integral dose and the volume receiving intermediate dose levels between IMRT and VMATI plans; 2) the use of 4D CT to determine the internal motion margin; and 3) evaluating the dosimetry of every plan through patient-specific QA. These factors may impact the overall treatment plan quality and outcomes from the individual planning technique used. In this study, we also examined the significance of using two arcs vs. a single-arc VMAT technique for PTV coverage, OARs doses, monitor units and delivery time. Thirteen patients, stage T2-T3 N0-N1 (TNM AJCC 7th edn.), PTV volume median 395 cc (range 281-601 cc), median age 69 years (range 53 to 85), were treated from July 2010 to June 2011 with a four-field (n = 4) or five-field (n = 9) step-and-shoot IMRT technique using a 6 MV beam to a prescribed dose of 50 Gy in 20 to 25 F. These patients were retrospectively replanned using single arc (VMATI, 91 control points) and two arcs (VMATII, 182 control points). All treatment plans of the 13 study cases were evaluated using various dose-volume metrics. These included PTV D99, PTV D95, PTV V9547.5Gy(95%), PTV mean dose, Dmax, PTV dose conformity (Van't Riet conformation number (CN)), mean lung dose, lung V20 and V5, liver V30, and Dmax to the spinal canal prv3mm. Also examined were the total plan monitor units (MUs) and the beam delivery time. Equivalent target coverage was observed with both VMAT single and two-arc plans. The comparison of VMATI with fixed-field IMRT demonstrated equivalent target coverage; statistically no significant difference were found in PTV D99 (p = 0.47), PTV mean (p = 0.12), PTV D95 and PTV V9547.5Gy (95%) (p = 0.38). However, Dmax in VMATI plans was significantly lower compared to IMRT (p = 0.02). The Van't Riet dose conformation number (CN) was also statistically in favor of VMATI plans (p = 0.04). VMATI achieved lower lung V20 (p = 0.05), whereas lung V5 (p = 0.35) and mean lung dose (p = 0.62) were not significantly different. The other OARs, including spinal canal, liver, heart, and kidneys showed no statistically significant differences between the two techniques. Treatment time delivery for VMATI plans was reduced by up to 55% (p = 5.8E-10) and MUs reduced by up to 16% (p = 0.001). Integral dose was not statistically different between the two planning techniques (p = 0.99). There were no statistically significant differences found in dose distribution of the two VMAT techniques (VMATI vs. VMATII) Dose statistics for both VMAT techniques were: PTV D99 (p = 0.76), PTV D95 (p = 0.95), mean PTV dose (p = 0.78), conformation number (CN) (p = 0.26), and MUs (p = 0.1). However, the treatment delivery time for VMATII increased significantly by two-fold (p = 3.0E-11) compared to VMATI. VMAT-based treatment planning is safe and deliverable for patients with thoracic esophageal cancer with similar planning goals, when compared to standard IMRT. The key benefit for VMATI was the reduction in treatment delivery time and MUs, and improvement in dose conformality. In our study, we found no significant difference in VMATII over single-arc VMATI for PTV coverage or OARs doses. However, we observed significant increase in delivery time for VMATII compared to VMATI.
Figures
Similar articles
-
Volumetric-modulated arc therapy vs. c-IMRT in esophageal cancer: a treatment planning comparison.World J Gastroenterol. 2012 Oct 7;18(37):5266-75. doi: 10.3748/wjg.v18.i37.5266. World J Gastroenterol. 2012. PMID: 23066322 Free PMC article.
-
Dosimetric comparison of TomoDirect, helical tomotherapy, VMAT, and ff-IMRT for upper thoracic esophageal carcinoma.Med Dosim. 2019 Summer;44(2):167-172. doi: 10.1016/j.meddos.2018.05.001. Epub 2018 Jun 24. Med Dosim. 2019. PMID: 29950277
-
Volumetric modulated arc therapy vs. c-IMRT for the treatment of upper thoracic esophageal cancer.PLoS One. 2015 Mar 27;10(3):e0121385. doi: 10.1371/journal.pone.0121385. eCollection 2015. PLoS One. 2015. PMID: 25815477 Free PMC article.
-
Hybrid Treatment Planning for Chest Wall Irradiation Utilizing Three-Dimensional Conformal Radiotherapy (3DCRT), Intensity-Modulated Radiation Therapy (IMRT), and Volumetric Modulated Arc Therapy (VMAT): A Systematic Review.Cureus. 2024 May 3;16(5):e59583. doi: 10.7759/cureus.59583. eCollection 2024 May. Cureus. 2024. PMID: 38832195 Free PMC article. Review.
-
Robust optimization in lung treatment plans accounting for geometric uncertainty.J Appl Clin Med Phys. 2018 May;19(3):19-26. doi: 10.1002/acm2.12291. Epub 2018 Mar 10. J Appl Clin Med Phys. 2018. PMID: 29524301 Free PMC article. Review.
Cited by
-
Clinical impact of magnetic resonance imaging distortions on gamma knife radiosurgery.J Med Radiat Sci. 2021 Sep;68(3):274-281. doi: 10.1002/jmrs.472. Epub 2021 May 4. J Med Radiat Sci. 2021. PMID: 33942565 Free PMC article.
-
An IMRT/VMAT Technique for Nonsmall Cell Lung Cancer.Biomed Res Int. 2015;2015:613060. doi: 10.1155/2015/613060. Epub 2015 Oct 11. Biomed Res Int. 2015. PMID: 26539515 Free PMC article.
-
Innovative regression model-based decision support tool for optimizing radiotherapy techniques in thoracic esophageal cancer.Front Oncol. 2024 Jul 24;14:1370293. doi: 10.3389/fonc.2024.1370293. eCollection 2024. Front Oncol. 2024. PMID: 39114310 Free PMC article.
-
What Is the Optimal Radiation Technique for Esophageal Cancer? A Dosimetric Comparison of Four Techniques.Cureus. 2018 Jul 16;10(7):e2985. doi: 10.7759/cureus.2985. Cureus. 2018. PMID: 30237946 Free PMC article.
-
VMAT planning study in rectal cancer patients.Radiat Oncol. 2014 Oct 16;9:219. doi: 10.1186/s13014-014-0219-1. Radiat Oncol. 2014. PMID: 25319073 Free PMC article.
References
-
- Callister MD. Radiotherapy for esophageal cancer, p. 141–159. In: Radiation Medical Rounds. New York: Demos Medical Publishing; 2010.
-
- La TH, Minn AY, Su Z. Multimodality treatment with intensity modulated radiation therapy for esophageal cancer. Dis Esophagus. 2010;23(4):300–08. - PubMed
-
- Palma DA, Verbakel WF, Otto K, Senan S. New developments in arc radiation therapy: a review. Cancer Treat Rev. 2010:36(5):393–99. - PubMed
-
- Wang X, Zhang X, Dong L, Liu H, Wu Q, Mohan R. Development of methods for beam angle optimization for IMRT using an accelerated exhaustive search strategy. Int J Radiat Oncol Biol Phys. 2004;60(4):1325–37. - PubMed
-
- van't Riet A, Mak AC, Moerland MA, Elders LH, van der Zee W. A conformation number to quantify the degree of conformality in brachytherapy and external beam irradiation: application to the prostate. Int J Radiat Oncol Biol Phys. 1997;37(3):731–36. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
