

Computed tomographic measures of pulmonary vascular morphology in smokers and their clinical implications
- PMID: 23656466
- PMCID: PMC3778757
- DOI: 10.1164/rccm.201301-0162OC
Computed tomographic measures of pulmonary vascular morphology in smokers and their clinical implications
Abstract
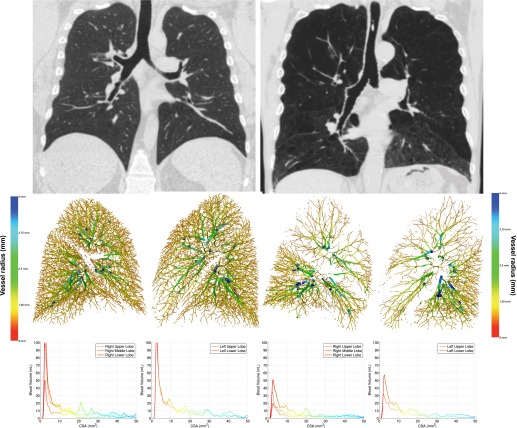
Rationale: Angiographic investigation suggests that pulmonary vascular remodeling in smokers is characterized by distal pruning of the blood vessels.
Objectives: Using volumetric computed tomography scans of the chest we sought to quantitatively evaluate this process and assess its clinical associations.
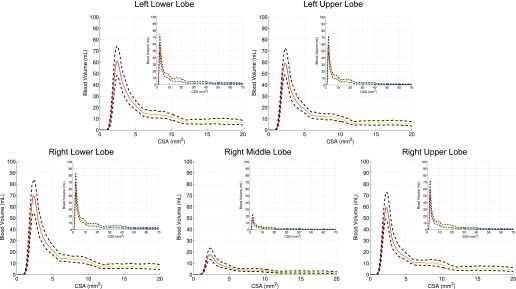
Methods: Pulmonary vessels were automatically identified, segmented, and measured. Total blood vessel volume (TBV) and the aggregate vessel volume for vessels less than 5 mm(2) (BV5) were calculated for all lobes. The lobe-specific BV5 measures were normalized to the TBV of that lobe and the nonvascular tissue volume (BV5/T(issue)V) to calculate lobe-specific BV5/TBV and BV5/T(issue)V ratios. Densitometric measures of emphysema were obtained using a Hounsfield unit threshold of -950 (%LAA-950). Measures of chronic obstructive pulmonary disease severity included single breath measures of diffusing capacity of carbon monoxide, oxygen saturation, the 6-minute-walk distance, St George's Respiratory Questionnaire total score (SGRQ), and the body mass index, airflow obstruction, dyspnea, and exercise capacity (BODE) index.
Measurements and main results: The %LAA-950 was inversely related to all calculated vascular ratios. In multivariate models including age, sex, and %LAA-950, lobe-specific measurements of BV5/TBV were directly related to resting oxygen saturation and inversely associated with both the SGRQ and BODE scores. In similar multivariate adjustment lobe-specific BV5/T(issue)V ratios were inversely related to resting oxygen saturation, diffusing capacity of carbon monoxide, 6-minute-walk distance, and directly related to the SGRQ and BODE.
Conclusions: Smoking-related chronic obstructive pulmonary disease is characterized by distal pruning of the small blood vessels (<5 mm(2)) and loss of tissue in excess of the vasculature. The magnitude of these changes predicts the clinical severity of disease.
Figures
References
-
- Chaouat A, Naeije R, Weitzenblum E. Pulmonary hypertension in COPD. Eur Respir J. 2008;32:1371–1385. - PubMed
-
- Minai OA, Chaouat A, Adnot S. Pulmonary hypertension in COPD: epidemiology, significance, and management: pulmonary vascular disease: the global perspective. Chest. 2010;137(Suppl. 6):39S–51S. - PubMed
-
- Oswald-Mammosser M, Weitzenblum E, Quoix E, Moser G, Chaouat A, Charpentier C, Kessler R. Prognostic factors in COPD patients receiving long-term oxygen therapy. Importance of pulmonary artery pressure. Chest. 1995;107:1193–1198. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 HL089897/HL/NHLBI NIH HHS/United States
- K23HL093351-04/HL/NHLBI NIH HHS/United States
- 2R01HL089897-06A1/HL/NHLBI NIH HHS/United States
- R01HL116473/HL/NHLBI NIH HHS/United States
- R01 HL116931/HL/NHLBI NIH HHS/United States
- R01 HL116473/HL/NHLBI NIH HHS/United States
- U01 HL089856/HL/NHLBI NIH HHS/United States
- 1R01HL116931-01/HL/NHLBI NIH HHS/United States
- 2R01HL089856-06A1/HL/NHLBI NIH HHS/United States
- K23 HL089353/HL/NHLBI NIH HHS/United States
- P50 HL107192/HL/NHLBI NIH HHS/United States
- K25 HL104085-03/HL/NHLBI NIH HHS/United States
- K25 HL104085/HL/NHLBI NIH HHS/United States
- P41 EB015902/EB/NIBIB NIH HHS/United States
- K23HL089353-05/HL/NHLBI NIH HHS/United States
- U01 HL089897/HL/NHLBI NIH HHS/United States
- K23 HL093351/HL/NHLBI NIH HHS/United States
- R01 HL089856/HL/NHLBI NIH HHS/United States
- K01 HL118714/HL/NHLBI NIH HHS/United States
- 1P50HL107192/HL/NHLBI NIH HHS/United States
- T32 HL105346/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
