

Recombinant HPA-1a antibody therapy for treatment of fetomaternal alloimmune thrombocytopenia: proof of principle in human volunteers
- PMID: 23656729
- PMCID: PMC3716198
- DOI: 10.1182/blood-2013-02-481887
Recombinant HPA-1a antibody therapy for treatment of fetomaternal alloimmune thrombocytopenia: proof of principle in human volunteers
Abstract
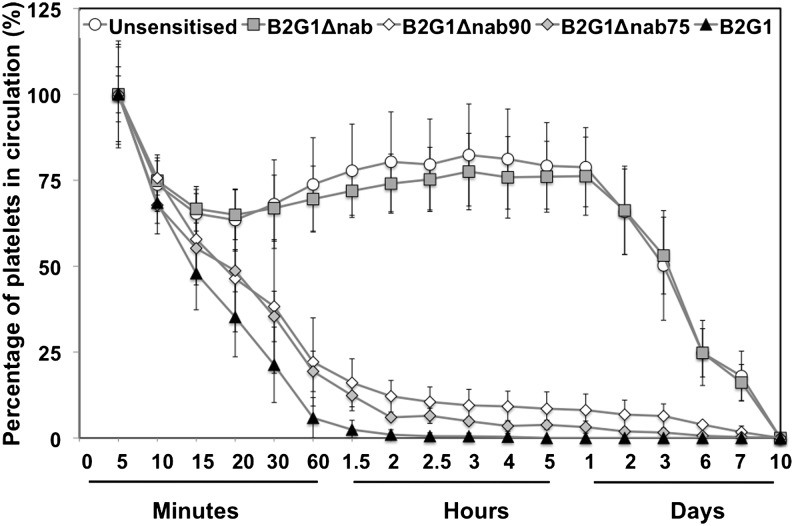
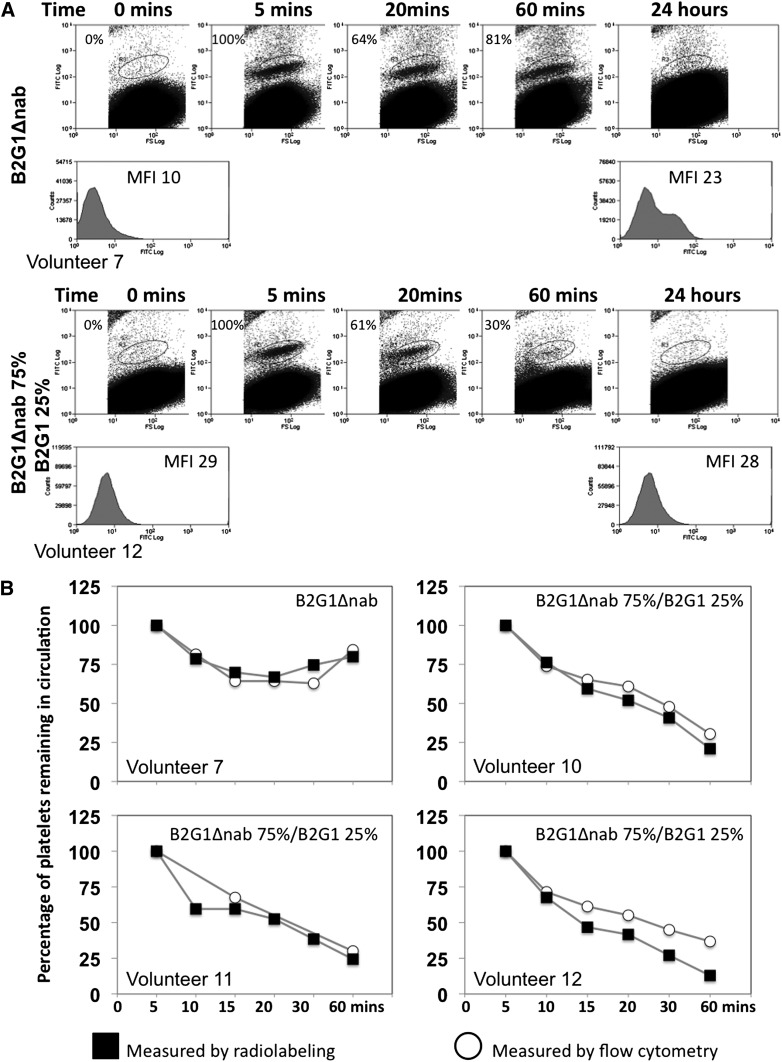
Fetomaternal alloimmune thrombocytopenia, caused by the maternal generation of antibodies against fetal human platelet antigen-1a (HPA-1a), can result in intracranial hemorrhage and intrauterine death. We have developed a therapeutic human recombinant high-affinity HPA-1a antibody (B2G1Δnab) that competes for binding to the HPA-1a epitope but carries a modified constant region that does not bind to Fcγ receptors. In vitro studies with a range of clinical anti-HPA-1a sera have shown that B2G1Δnab blocks monocyte chemiluminescence by >75%. In this first-in-man study, we demonstrate that HPA-1a1b autologous platelets (matching fetal phenotype) sensitized with B2G1Δnab have the same intravascular survival as unsensitized platelets (190 hours), while platelets sensitized with a destructive immunoglobulin G1 version of the antibody (B2G1) are cleared from the circulation in 2 hours. Mimicking the situation in fetuses receiving B2G1Δnab as therapy, we show that platelets sensitized with a combination of B2G1 (representing destructive HPA-1a antibody) and B2G1Δnab survive 3 times as long in circulation compared with platelets sensitized with B2G1 alone. This confirms the therapeutic potential of B2G1Δnab. The efficient clearance of platelets sensitized with B2G1 also opens up the opportunity to carry out studies of prophylaxis to prevent alloimmunization in HPA-1a-negative mothers.
Figures
Comment in
-
Modified antibody in fetal alloimmunization.Blood. 2013 Jul 18;122(3):303-4. doi: 10.1182/blood-2013-05-502625. Blood. 2013. PMID: 23869072
References
-
- Hohlfeld P, Forestier F, Kaplan C, Tissot JD, Daffos F. Fetal thrombocytopenia: a retrospective survey of 5,194 fetal blood samplings. Blood. 1994;84(6):1851–1856. - PubMed
-
- Bussel JB, Zabusky MR, Berkowitz RL, McFarland JG. Fetal alloimmune thrombocytopenia. N Engl J Med. 1997;337(1):22–26. - PubMed
-
- Williamson LM, Hackett G, Rennie J, et al. The natural history of fetomaternal alloimmunization to the platelet-specific antigen HPA-1a (PlA1, Zwa) as determined by antenatal screening. Blood. 1998;92(7):2280–2287. - PubMed
-
- Kjeldsen-Kragh J, Killie MK, Tomter G, et al. A screening and intervention program aimed to reduce mortality and serious morbidity associated with severe neonatal alloimmune thrombocytopenia. Blood. 2007;110(3):833–839. - PubMed
-
- Mueller-Eckhardt C, Kiefel V, Grubert A, et al. 348 cases of suspected neonatal alloimmune thrombocytopenia. Lancet. 1989;1(8634):363–366. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
