

The natural history of secondary muscle-invasive bladder cancer
- PMID: 23656972
- PMCID: PMC3655874
- DOI: 10.1186/1471-2490-13-23
The natural history of secondary muscle-invasive bladder cancer
Abstract
Background: The management of patients with high-grade non muscle invasive bladder cancer (NMIBC) brings diagnostic and therapeutic challenges. In the current study, we sought to study the natural history of progression to "secondary" muscle-invasive bladder cancer (MIBC)-cancer that developed during follow up of patients presenting with non-muscle invasive bladder cancer (NMIBC).
Methods: Between 1998 and 2008, 760 patients were treated for bladder cancer. Primary MIBC (>=T2) tumors (present upon presentation) were diagnosed in 114 patients. All patients with high-grade NMIBC were treated with intravesical BCG. Mean follow-up was 44 months.
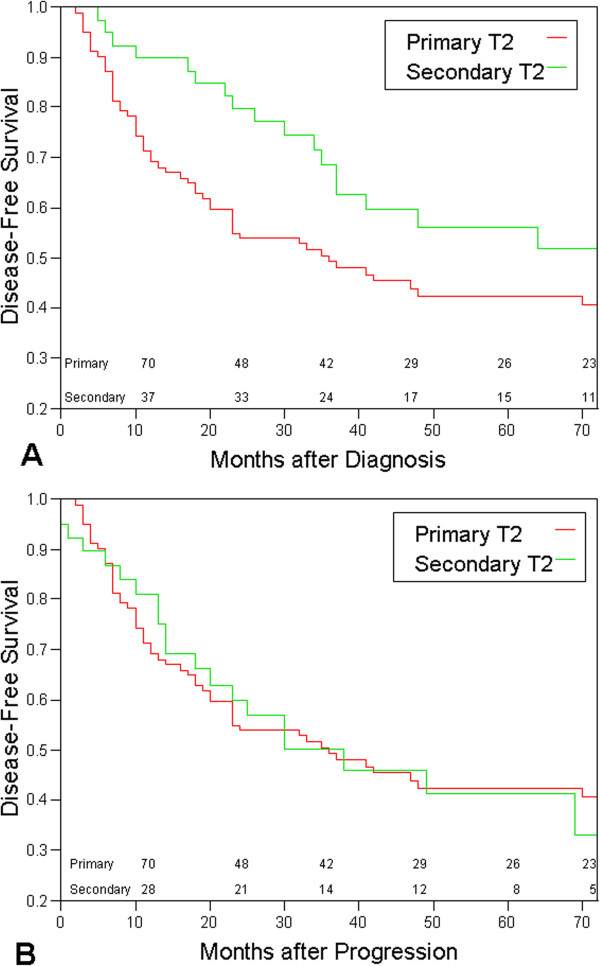
Results: Forty patients (6.1%) developed secondary MIBC after a mean period of 21 months from initial diagnosis of bladder cancer. The 2- and 5-year disease-specific survival rates were better for patients with secondary MIBC (90% and 56% compared to 69% and 42% for patients with primary disease, p=0.03). The Kaplan-Meier curves of the two groups were parallel but displaced by approximately 2 years.
Conclusion: In the current series, MIBC progression occurred among initially presenting patients with NMIBC in 6.1%. In most patients, the initial diagnosis of NMIBC is correct and muscle invasion occurs after a mean period of about 2 years. This supports a non-radical approach in patients with high-grade T1, Ta or Tis. Meticulous follow-up with liberal biopsy of any suspicious lesion may provide early diagnosis of invasive disease.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
