

Reliability of overcoverage parameters with varying morphologic pincer features: comparison of EOS® and radiography
- PMID: 23657877
- PMCID: PMC3705041
- DOI: 10.1007/s11999-013-3001-z
Reliability of overcoverage parameters with varying morphologic pincer features: comparison of EOS® and radiography
Abstract
Background: Multiple radiographic parameters used for diagnosis and quantification of morphologic pincer features have emerged, but the degree to which pelvic tilt or rotation affects conventional radiography and EOS(®) is unknown.
Question/purposes: We asked: (1) What is the reliability of EOS(®) and conventional radiography at increasing sizes of morphologic pincer features with varying degrees of tilt and rotation? (2) What is the effect of tilt and rotation on acetabular overcoverage measurements?
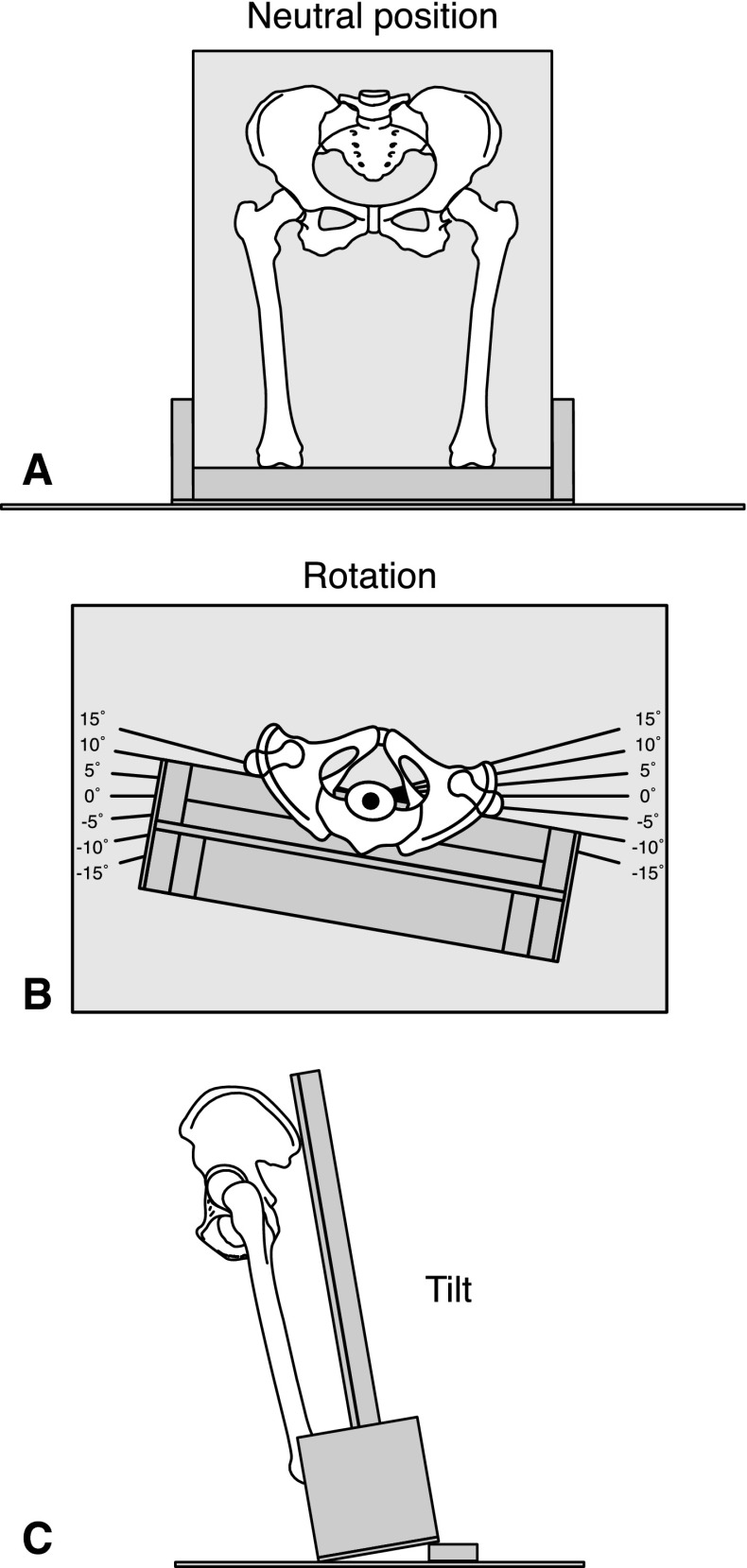
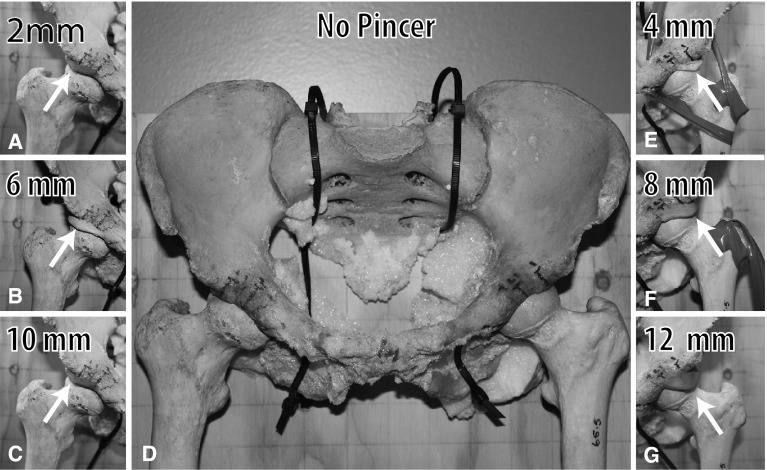
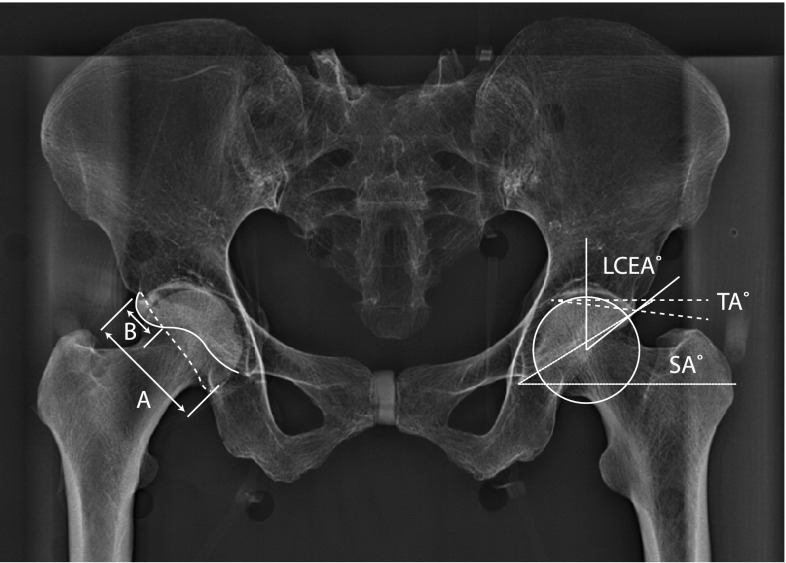
Methods: Using a dry cadaveric pelvis, AP conventional radiographs and EOS(®) images were taken at intervals of increasing modeled pincer size with 0° to 15° varying tilt and rotation. Lateral center-edge angle, Sharp angle, Tönnis angle, crossover sign, and retroversion index were measured on all images. Statistical analysis was conducted.
Results: The intermodality intraclass correlation coefficients for conventional radiography and EOS(®) radiography across all pincer sizes, rotations, and tilts were excellent (0.93-0.98). Crossover sign was in perfect agreement in conventional radiography and EOS(®). Rotation of the hip away from the beam source and/or increased anterior tilt falsely increased all overcoverage parameters except for Tönnis angle. Rotation away from the beam of 10° or greater or anterior tilt of 5° or greater produced a false-positive crossover sign.
Conclusions: EOS(®) radiography maintained excellent reliability in comparison to conventional radiography but both were equally vulnerable to the effects of tilt and rotation for quantification of hip parameters used in acetabular overcoverage assessment. A standardized pelvic radiograph ensuring that the pelvis is not excessively tilted or rotated should be used for assessing acetabular overcoverage parameters.
Figures


Similar articles
-
Which radiographic hip parameters do not have to be corrected for pelvic rotation and tilt?Clin Orthop Relat Res. 2015 Apr;473(4):1255-66. doi: 10.1007/s11999-014-3936-8. Clin Orthop Relat Res. 2015. PMID: 25231153 Free PMC article.
-
Supine and Standing AP Pelvis Radiographs in the Evaluation of Pincer Femoroacetabular Impingement.Clin Orthop Relat Res. 2016 Jul;474(7):1692-6. doi: 10.1007/s11999-016-4766-7. Epub 2016 Feb 25. Clin Orthop Relat Res. 2016. PMID: 26913511 Free PMC article.
-
A quantitative method to assess focal acetabular overcoverage resulting from pincer deformity using CT data.Clin Orthop Relat Res. 2011 Oct;469(10):2846-54. doi: 10.1007/s11999-011-1958-z. Epub 2011 Jul 12. Clin Orthop Relat Res. 2011. PMID: 21748515 Free PMC article.
-
Acetabular Rim Disorders/Pincer-type Femoroacetabular Impingement and Hip Arthroscopy.Sports Med Arthrosc Rev. 2021 Mar 1;29(1):35-43. doi: 10.1097/JSA.0000000000000296. Sports Med Arthrosc Rev. 2021. PMID: 33395229 Review.
-
The Reliability of Commonly Used Radiographic Parameters in the Evaluation of the Pre-Arthritic Hip: A Systematic Review.JBJS Rev. 2019 Feb;7(2):e3. doi: 10.2106/JBJS.RVW.18.00048. JBJS Rev. 2019. PMID: 30762702
Cited by
-
"Simple mechanical devices did not improve pelvis positioning in AP pelvis radiographs for reliable assessment of the acetabular orientation".J Exp Orthop. 2019 May 23;6(1):20. doi: 10.1186/s40634-019-0191-7. J Exp Orthop. 2019. PMID: 31123936 Free PMC article.
-
Effects of pelvic obliquity and limb position on radiographic leg length discrepancy measurement: a Sawbones model.J Exp Orthop. 2022 Jul 26;9(1):71. doi: 10.1186/s40634-022-00506-7. J Exp Orthop. 2022. PMID: 35881204 Free PMC article.
-
Which radiographic hip parameters do not have to be corrected for pelvic rotation and tilt?Clin Orthop Relat Res. 2015 Apr;473(4):1255-66. doi: 10.1007/s11999-014-3936-8. Clin Orthop Relat Res. 2015. PMID: 25231153 Free PMC article.
-
Impact of Femoroacetabular Impingement Morphology on Gait Assessment in Symptomatic Patients.Sports Health. 2015 Sep-Oct;7(5):429-36. doi: 10.1177/1941738115592827. Epub 2015 Jun 25. Sports Health. 2015. PMID: 26502419 Free PMC article.
-
Supine and Standing AP Pelvis Radiographs in the Evaluation of Pincer Femoroacetabular Impingement.Clin Orthop Relat Res. 2016 Jul;474(7):1692-6. doi: 10.1007/s11999-016-4766-7. Epub 2016 Feb 25. Clin Orthop Relat Res. 2016. PMID: 26913511 Free PMC article.
References
-
- Bell AL, Brand RA. Roentgenographic changes in proximal femoral dimensions due to hip rotation. Clin Orthop Relat Res. 1989;240:194–199. - PubMed
-
- Bushberg JT. The Essential Physics of Medical Imaging. Philadelphia, PA: Lippincott Williams & Wilkins; 2002.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
