

Spectrum of injuries associated with paediatric ACL tears: an MRI pictorial review
- PMID: 23657940
- PMCID: PMC3675256
- DOI: 10.1007/s13244-013-0250-z
Spectrum of injuries associated with paediatric ACL tears: an MRI pictorial review
Abstract
Objective: Magnetic resonance imaging (MRI) findings in anterior cruciate ligament (ACL) injury are well known, but most published reviews show obvious examples of associated injuries and give little focus to paediatric patients. Here, we demonstrate the spectrum of MRI appearances at common sites of associated injury in adolescents with ACL tears, emphasising age-specific issues.
Methods: Pictorial review using images from children with surgically confirmed ACL tears after athletic injury.
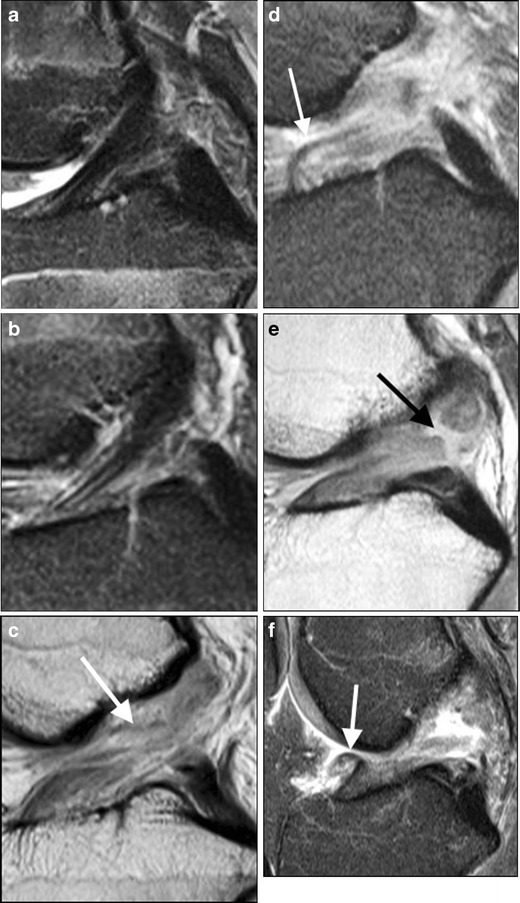
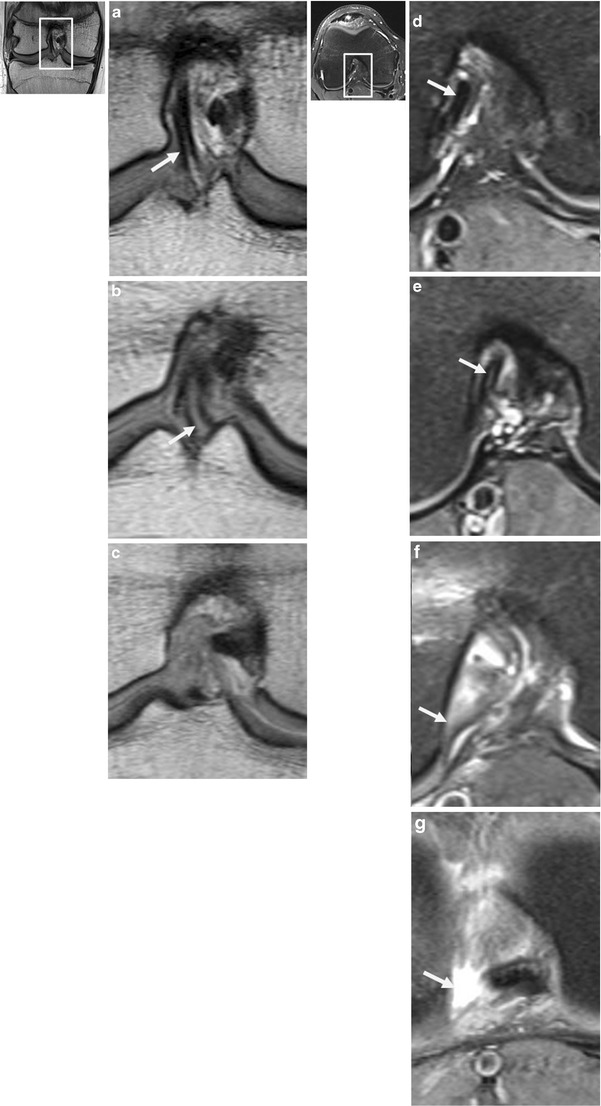
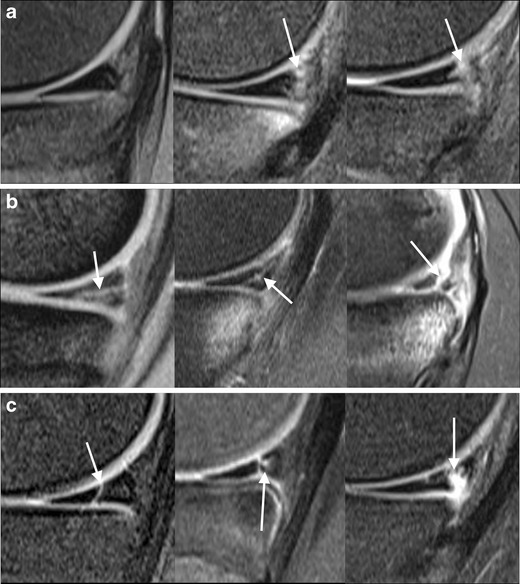
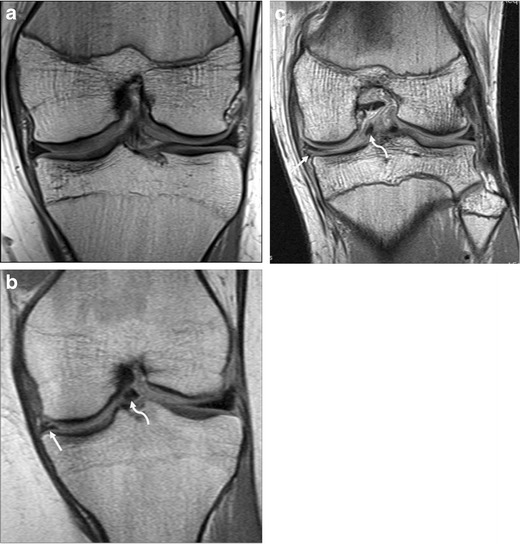
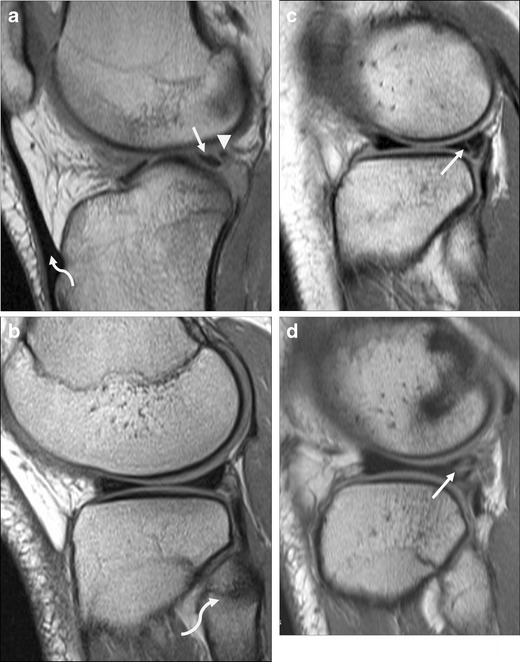
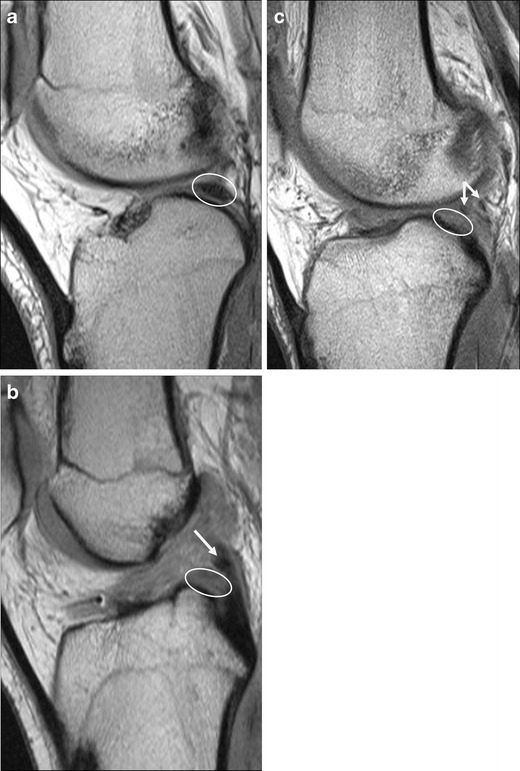
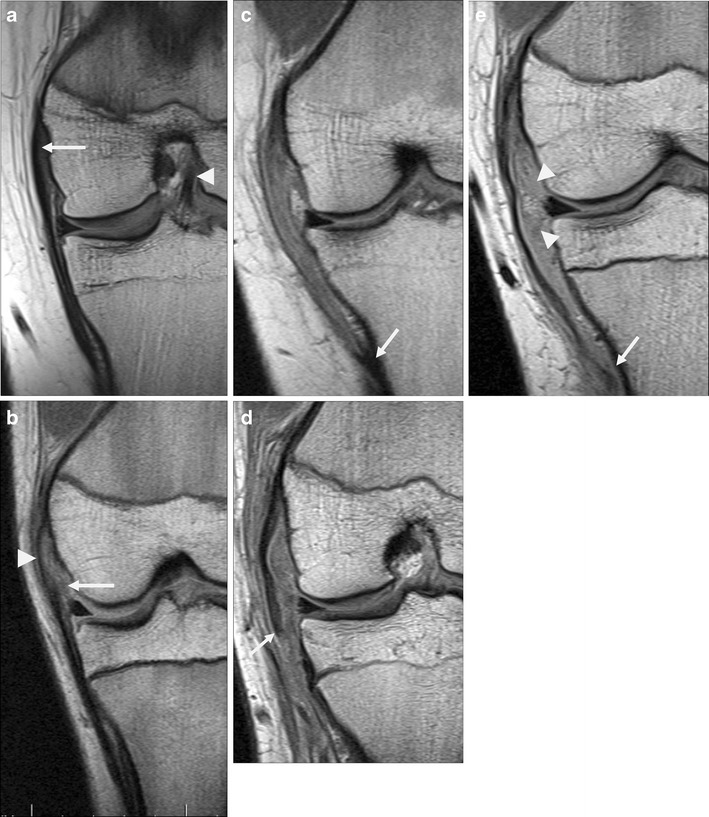
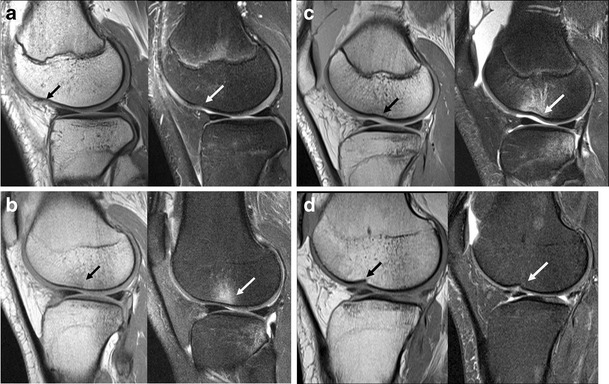
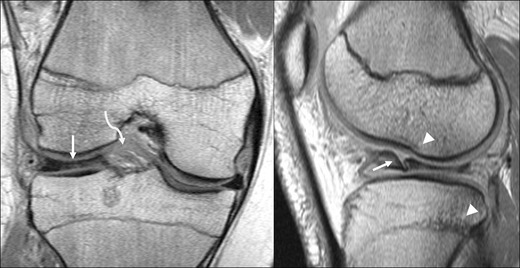
Results: ACL injury usually occurs with axial rotation in the valgus near full extension. The MRI findings can be obvious and important to management (ACL rupture), subtle but clinically important (lateral meniscus posterior attachment avulsion), obvious and unimportant to management (femoral condyle impaction injury), or subtle and possibly important (medial meniscocapsular junction tear). Paediatric-specific issues of note include tibial spine avulsion, normal difficulty visualising a thin ACL and posterolateral corner structures, and differentiation between incompletely closed physis and impaction fracture.
Conclusion: ACL tear is only the most obvious sign of a complex injury involving multiple structures. Awareness of the spectrum of secondary findings illustrated here and the features distinguishing them from normal variation can aid in accurate assessment of ACL tears and related injuries, enabling effective treatment planning and assessment of prognosis.
Teaching points: • The ACL in children normally appears thin or attenuated, while thickening and oedema suggest tear. • Displaced medial meniscal tears are significantly more common later post-injury than immediately. • The meniscofemoral ligaments merge with the posterior lateral meniscus, complicating tear assessment. • Tibial plateau impaction fractures can be difficult to distinguish from a partially closed physis. • Axial MR sequences are more sensitive/specific than coronal for diagnosis of medial collateral ligament (MCL) injury.
Figures



Similar articles
-
Incidence of Displaced Posterolateral Tibial Plateau and Lateral Femoral Condyle Impaction Fractures in the Setting of Primary Anterior Cruciate Ligament Tear.Am J Sports Med. 2020 Mar;48(3):545-553. doi: 10.1177/0363546519895239. Epub 2020 Jan 9. Am J Sports Med. 2020. PMID: 31917606
-
Morphologic Variants of Posterolateral Tibial Plateau Impaction Fractures in the Setting of Primary Anterior Cruciate Ligament Tear.Am J Sports Med. 2020 Feb;48(2):318-325. doi: 10.1177/0363546519893709. Epub 2020 Jan 3. Am J Sports Med. 2020. PMID: 31899869
-
The Incidence of Posterolateral Tibial Plateau and Central Lateral Femoral Condylar Impaction Fractures in a Pediatric and Young Adult Population.J Pediatr Orthop. 2023 Jan 1;43(1):18-23. doi: 10.1097/BPO.0000000000002270. Epub 2022 Sep 21. J Pediatr Orthop. 2023. PMID: 36129359
-
Associated injuries in pediatric and adolescent anterior cruciate ligament tears: does a delay in treatment increase the risk of meniscal tear?Arthroscopy. 2002 Nov-Dec;18(9):955-9. doi: 10.1053/jars.2002.36114. Arthroscopy. 2002. PMID: 12426537 Review.
-
Association of Tibial Plateau Fracture Morphology With Ligament Disruption in the Context of Multiligament Knee Injury.Curr Probl Diagn Radiol. 2018 Nov;47(6):410-416. doi: 10.1067/j.cpradiol.2017.09.001. Epub 2017 Sep 12. Curr Probl Diagn Radiol. 2018. PMID: 28992997 Review.
Cited by
-
The lateral femoral notch sign: a reliable diagnostic measurement in acute anterior cruciate ligament injury.Knee Surg Sports Traumatol Arthrosc. 2019 Feb;27(2):659-664. doi: 10.1007/s00167-018-5214-x. Epub 2018 Oct 13. Knee Surg Sports Traumatol Arthrosc. 2019. PMID: 30317524 Free PMC article.
-
Bone Bruise Patterns Associated With Pediatric and Adult Anterior Cruciate Ligament Tears Are Different.Arthrosc Sports Med Rehabil. 2022 Dec 28;5(1):e151-e157. doi: 10.1016/j.asmr.2022.11.006. eCollection 2023 Feb. Arthrosc Sports Med Rehabil. 2022. PMID: 36866294 Free PMC article.
-
Intrasubstance Anterior Cruciate Ligament Injuries in the Pediatric Population.Indian J Orthop. 2018 Sep-Oct;52(5):513-521. doi: 10.4103/ortho.IJOrtho_381_17. Indian J Orthop. 2018. PMID: 30237609 Free PMC article.
-
Sensitivity and Specificity of MRI in Diagnosing Concomitant Meniscal Injuries With Pediatric and Adolescent Acute ACL Tears.Orthop J Sports Med. 2022 Mar 9;10(3):23259671221079338. doi: 10.1177/23259671221079338. eCollection 2022 Mar. Orthop J Sports Med. 2022. PMID: 35295551 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
