

Drug repurposing for gastrointestinal stromal tumor
- PMID: 23657945
- PMCID: PMC3707936
- DOI: 10.1158/1535-7163.MCT-12-0968
Drug repurposing for gastrointestinal stromal tumor
Abstract
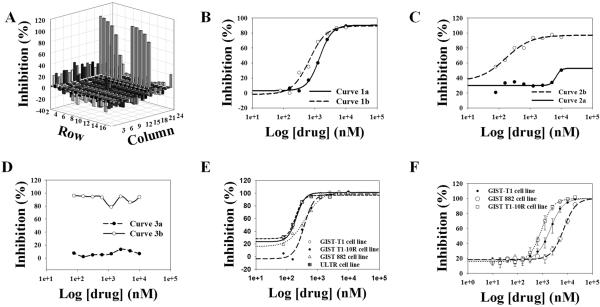
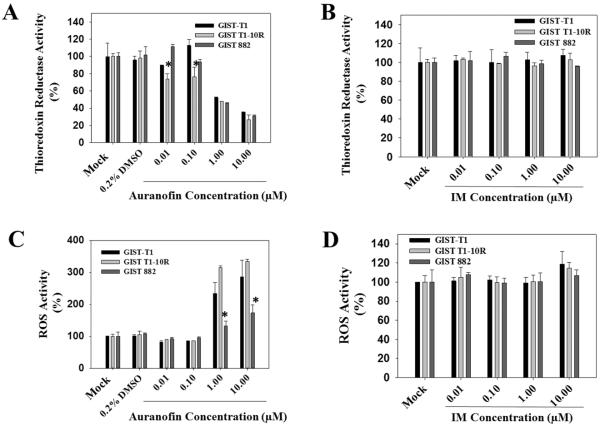
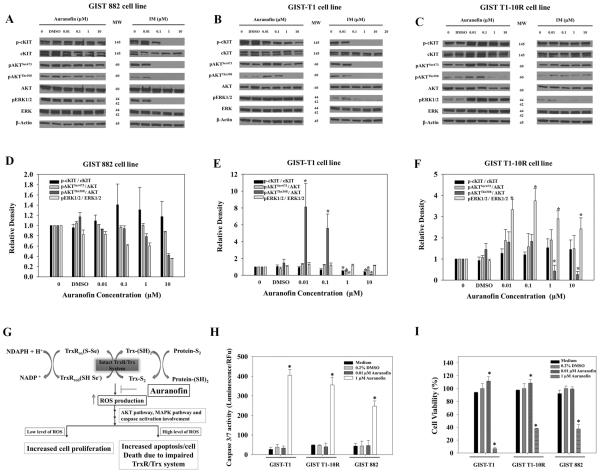
Despite significant treatment advances over the past decade, metastatic gastrointestinal stromal tumor (GIST) remains largely incurable. Rare diseases, such as GIST, individually affect small groups of patients but collectively are estimated to affect 25 to 30 million people in the United States alone. Given the costs associated with the discovery, development, and registration of new drugs, orphan diseases such as GIST are often not pursued by mainstream pharmaceutical companies. As a result, "drug repurposing" or "repositioning," has emerged as an alternative to the traditional drug development process. In this study, we screened 796 U.S. Food and Drug Administration (FDA)-approved drugs and found that two of these compounds, auranofin (Ridaura) and fludarabine phosphate, effectively and selectively inhibited the proliferation of GISTs, including imatinib-resistant cells. One of the most notable drug hits, auranofin, an oral, gold-containing agent approved by the FDA in 1985 for the treatment of rheumatoid arthritis, was found to inhibit thioredoxin reductase activity and induce reactive oxygen species (ROS) production, leading to dramatic inhibition of GIST cell growth and viability. Importantly, the anticancer activity associated with auranofin was independent of imatinib-resistant status, but was closely related to the endogenous and inducible levels of ROS. Coupled with the fact that auranofin has an established safety profile in patients, these findings suggest for the first time that auranofin may have clinical benefit for patients with GIST, particularly in those suffering from imatinib-resistant and recurrent forms of this disease.
Figures
References
-
- Corless CL, Heinrich MC. Molecular pathobiology of gastrointestinal stromal sarcomas. Annu Rev Pathol. 2008;3:557–86. - PubMed
-
- Hirota S, Isozaki K, Moriyama Y, Hashimoto K, Nishida T, Ishiguro S, et al. Gain-of-function mutations of c-kit in human gastrointestinal stromal tumors. Science. 1998;279:577–80. - PubMed
-
- Heinrich MC, Corless CL, Duensing A, McGreevey L, Chen CJ, Joseph N, et al. PDGFRA activating mutations in gastrointestinal stromal tumors. Science. 2003;299:708–10. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
