

Future of cholesteryl ester transfer protein (CETP) inhibitors: a pharmacological perspective
- PMID: 23658137
- PMCID: PMC3720705
- DOI: 10.1007/s40262-013-0071-8
Future of cholesteryl ester transfer protein (CETP) inhibitors: a pharmacological perspective
Abstract
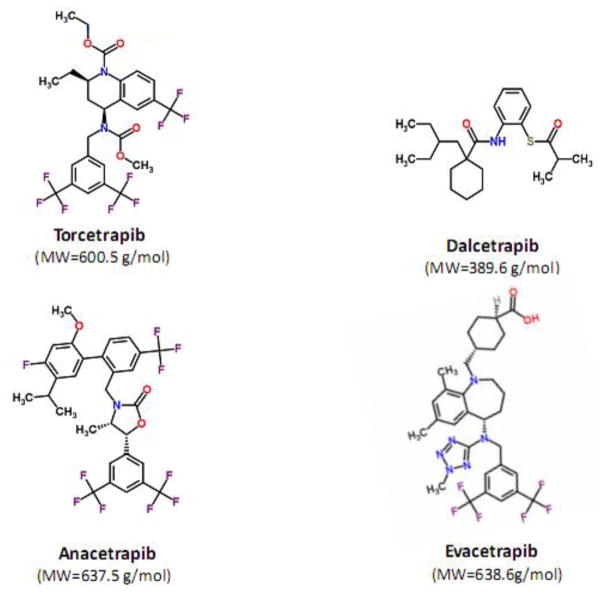
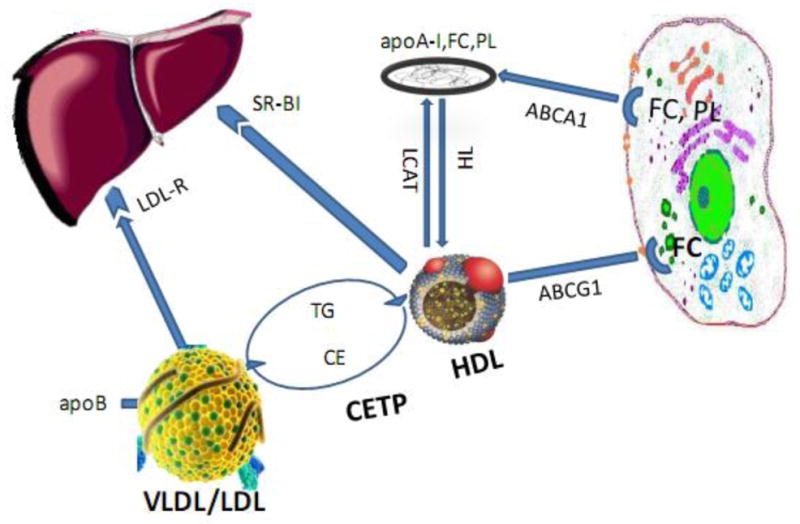
In almost 30 years since the introduction of HMG-CoA reductase inhibitors (statins), no other class of lipid modulators has entered the market. Elevation of high-density lipoprotein-cholesterol (HDL-C) via inhibiting cholesteryl ester transfer protein (CETP) is an attractive strategy for reducing the risk of cardiovascular events in high-risk patients. Transfer of triglyceride and cholesteryl ester (CE) between lipoproteins is mediated by CETP; thus inhibition of this pathway can increase the concentration of HDL-C. Torcetrapib was the first CETP inhibitor evaluated in phase III clinical trials. Because of off-target effects, torcetrapib raised blood pressure and increased the concentration of serum aldosterone, leading to higher cardiovascular events and mortality. Torcetrapib showed positive effects on cardiovascular risk especially in patients with a greater increase in HDL-C and apolipoprotein A-1 (apoA-1) levels. The phase III clinical trial of dalcetrapib, the second CETP inhibitor that has entered clinical development, was terminated because of ineffectiveness. Dalcetrapib is a CETP modulator that elevated HDL-C levels but did not reduce the concentration of low-density lipoprotein cholesterol (LDL-C). Both heterotypic and homotypic CE transfer between lipoproteins are mediated by some CETP inhibitors, including torcetrapib, anacetrapib, and evacetrapib, while dalcetrapib only affects the heterotypic CE transfer. Dalcetrapib has a chemical structure that is distinct from other CETP inhibitors, with a smaller molecular weight and a lack of trifluoride moieties. Moreover, dalcetrapib is a pro-drug that must be hydrolyzed to a pharmacologically active thiol form. Two other CETP inhibitors, anacetrapib and evacetrapib, are currently undergoing evaluation in phase III clinical trials. Both molecules have shown beneficial effects by increasing HDL-C and decreasing LDL-C concentration. The success of anacetrapib and evacetrapib remains to be confirmed upon the completion of phase III clinical trials in 2017 and 2015, respectively. Generally, the concentration of HDL-C has been considered a biomarker for the activity of CETP inhibitors. However, it is not clear whether a fundamental relationship exists between HDL-C levels and the risk of coronary artery diseases. The most crucial role for HDL is cholesterol efflux capacity in which HDL can reverse transport cholesterol from foam cells in atherosclerotic plaques. In view of the heterogeneity in HDL particle size, charge, and composition, the mere concentration of HDL-C may not be a good surrogate marker for HDL functionality. Recent clinical studies have reported that increased HDL functionality inversely correlates with the development of atherosclerotic plaque. Future development of CETP inhibitors may therefore benefit from the use of biomarkers of HDL functionality.
Conflict of interest statement
The authors (Mohammadpour AH and Akhlaghi F) declare no conflicts of interest.
Figures
References
-
- Gordon T, Castelli WP, Hjortland MC, et al. High density lipoprotein as a protective factor against coronary heart disease. the Framingham study. Am J Med. 1977 May;62(5):707–14. - PubMed
-
- Castelli WP, Garrison RJ, Wilson PW, et al. Incidence of coronary heart disease and lipoprotein cholesterol levels. The Framingham Study. JAMA. 1986 Nov 28;256(20):2835–8. - PubMed
-
- Corti MC, Guralnik JM, Salive ME, et al. HDL cholesterol predicts coronary heart disease mortality in older persons. JAMA. 1995 Aug 16;274(7):539–44. - PubMed
-
- Gordon DJ, Probstfield JL, Garrison RJ, et al. High-density lipoprotein cholesterol and cardiovascular disease. Four prospective American studies. Circulation. 1989 Jan;79(1):8–15. - PubMed
-
- Kuvin JT, Alsheikh-Ali AA, Karas RH. High-density lipoprotein cholesterol-raising strategies. J Cardiovasc Pharmacol. 2006 Feb;47(2):196–204. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
