

doi: 10.1158/2159-8290.CD-13-0131.
Deja Vu: EGF receptors drive resistance to BRAF inhibitors
Affiliations
- PMID: 23658295
- PMCID: PMC3736320
- DOI: 10.1158/2159-8290.CD-13-0131
Item in Clipboard
Deja Vu: EGF receptors drive resistance to BRAF inhibitors
Cancer Discov.
2013 May.
Abstract
The promise of personalized medicine is upon us, and in some cancers, targeted therapies are rapidly becoming the mainstay of treatment for selected patients based on their molecular profile. The protein kinase BRAF is a driver oncogene in both thyroid cancer and melanoma, but while drugs that target BRAF and its downstream signaling pathway are effective in melanoma, they are ineffective in thyroid cancer. In this issue of Cancer Discovery, Montero-Conde and colleagues investigate why thyroid cancer is resistant to BRAF inhibitors despite the presence of BRAF mutation.
Figures
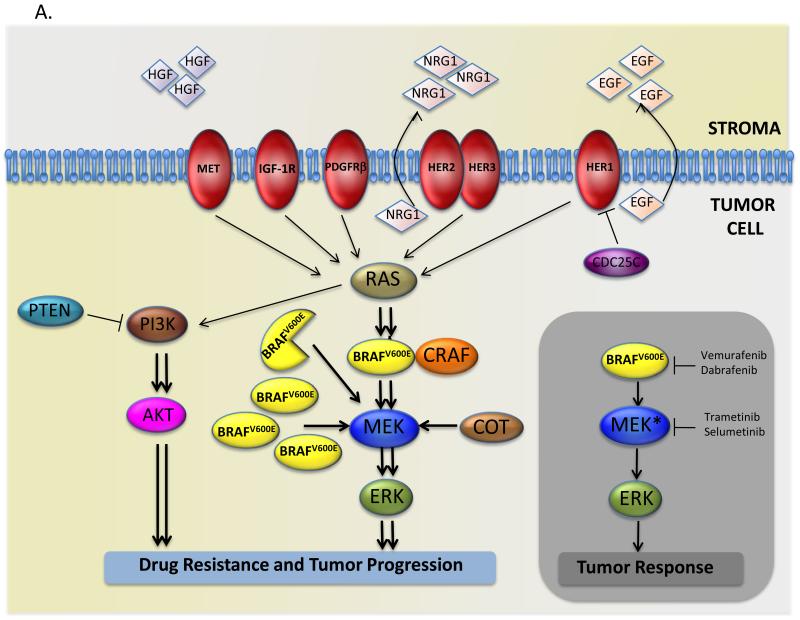
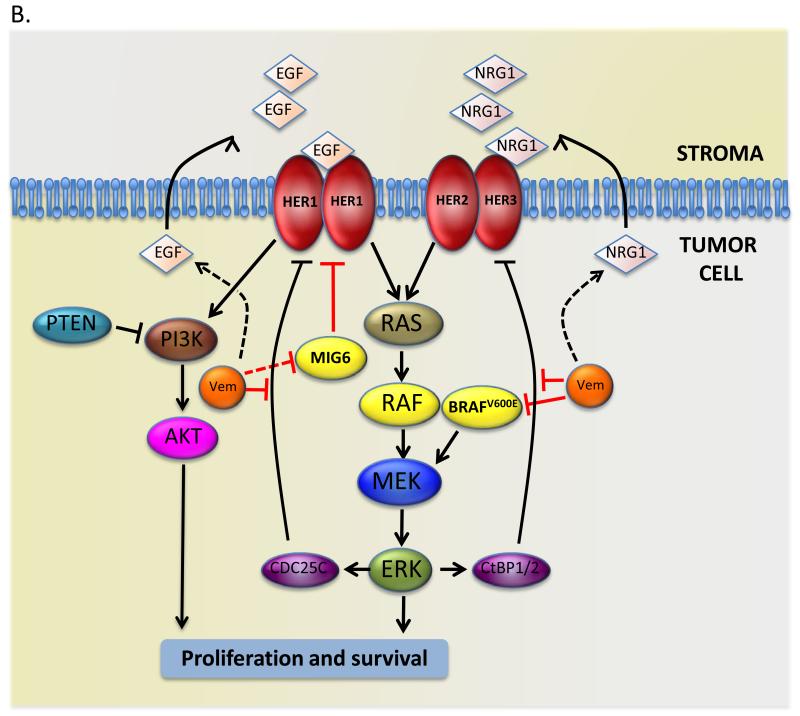
(A) Grey rectangle: mutant BRAF (BRAFV600E) hyper-activates ERK signaling and promotes tumor cell proliferation and survival, but BRAF and MEK drugs inhibit the pathway and block tumor progression. Main figure: resistance to BRAF inhibitors is mediated by several mechanisms, including expression of a truncated forms of mutant BRAF, increased expression of mutant BRAF or wild-type CRAF, acquisition of mutations in RAS or MEK, expression of MAP3K8/COT, loss of PTEN expression, or activation of the receptor tyrosine kinases PDGFRβ, IGF-1R, EGFR and HER2/HER3, or increased activation of MET through the increased secretion of HGF by the stromal compartment. (B) EGF family receptors mediate resistance to BRAF inhibitors. In colorectal cells BRAF inhibits HER1 by inducing CDC25C, so BRAF inhibition by vemurafenib (Vem) releases the block to HER1 activation by reducing CDC25C expression. In thyroid cancer cells HER3 expression is inhibited by BRAF through the CtBP1/2 transcription repressors, so BRAF inhibition by vemurafenib (Vem) results in increased HER3 expression, and it alsoincreases NRG1 expression through unknown mechanisms. In melanoma, BRAF inhibition by vemurafenib (Vem) drives HER1 signaling by increasing EGF secretion, increasing HER1 expression and suppressing MIG6 activity through unknown mechanisms.
(A) Grey rectangle: mutant BRAF (BRAFV600E) hyper-activates ERK signaling and promotes tumor cell proliferation and survival, but BRAF and MEK drugs inhibit the pathway and block tumor progression. Main figure: resistance to BRAF inhibitors is mediated by several mechanisms, including expression of a truncated forms of mutant BRAF, increased expression of mutant BRAF or wild-type CRAF, acquisition of mutations in RAS or MEK, expression of MAP3K8/COT, loss of PTEN expression, or activation of the receptor tyrosine kinases PDGFRβ, IGF-1R, EGFR and HER2/HER3, or increased activation of MET through the increased secretion of HGF by the stromal compartment. (B) EGF family receptors mediate resistance to BRAF inhibitors. In colorectal cells BRAF inhibits HER1 by inducing CDC25C, so BRAF inhibition by vemurafenib (Vem) releases the block to HER1 activation by reducing CDC25C expression. In thyroid cancer cells HER3 expression is inhibited by BRAF through the CtBP1/2 transcription repressors, so BRAF inhibition by vemurafenib (Vem) results in increased HER3 expression, and it alsoincreases NRG1 expression through unknown mechanisms. In melanoma, BRAF inhibition by vemurafenib (Vem) drives HER1 signaling by increasing EGF secretion, increasing HER1 expression and suppressing MIG6 activity through unknown mechanisms.
Comment in
-
Relief of feedback inhibition of HER3 transcription by RAF and MEK inhibitors attenuates their antitumor effects in BRAF-mutant thyroid carcinomas.Cancer Discov. 2013 May;3(5):520-33. doi: 10.1158/2159-8290.CD-12-0531. Epub 2013 Jan 29. Cancer Discov. 2013. PMID: 23365119 Free PMC article.
References
-
- Davies H, Bignell GR, Cox C, Stephens P, Edkins S, Clegg S, et al. Mutations of the BRAF gene in human cancer. Nature. 2002;417:949–54. - PubMed
-
- Hauschild A, Grob JJ, Demidov LV, Jouary T, Gutzmer R, Millward M, et al. Dabrafenib in BRAF-mutated metastatic melanoma: a multicentre, open-label, phase 3 randomised controlled trial. Lancet. 2012;380:358–65. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
