

Occurrence of vasospasm and infarction in relation to a focal monitoring sensor in patients after SAH: placing a bet when placing a probe?
- PMID: 23658768
- PMCID: PMC3642192
- DOI: 10.1371/journal.pone.0062754
Occurrence of vasospasm and infarction in relation to a focal monitoring sensor in patients after SAH: placing a bet when placing a probe?
Abstract
Introduction: Vasospastic brain infarction is a devastating complication of aneurysmal subarachnoid hemorrhage (SAH). Using a probe for invasive monitoring of brain tissue oxygenation or blood flow is highly focal and may miss the site of cerebral vasospasm (CVS). Probe placement is based on the assumption that the spasm will occur either at the dependent vessel territory of the parent artery of the ruptured aneurysm or at the artery exposed to the focal thick blood clot. We investigated the likelihood of a focal monitoring sensor being placed in vasospasm or infarction territory on a hypothetical basis.
Methods: From our database we retrospectively selected consecutive SAH patients with angiographically proven (day 7-14) severe CVS (narrowing of vessel lumen >50%). Depending on the aneurysm location we applied a standard protocol of probe placement to detect the most probable site of severe CVS or infarction. We analyzed whether the placement was congruent with existing CVS/infarction.
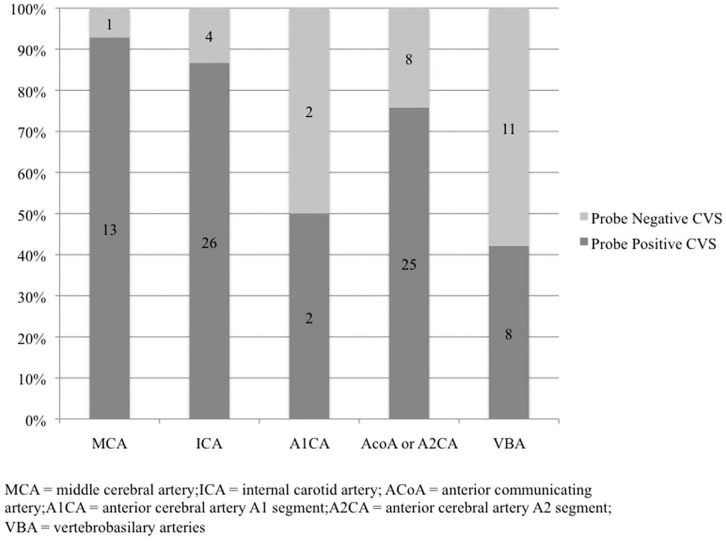
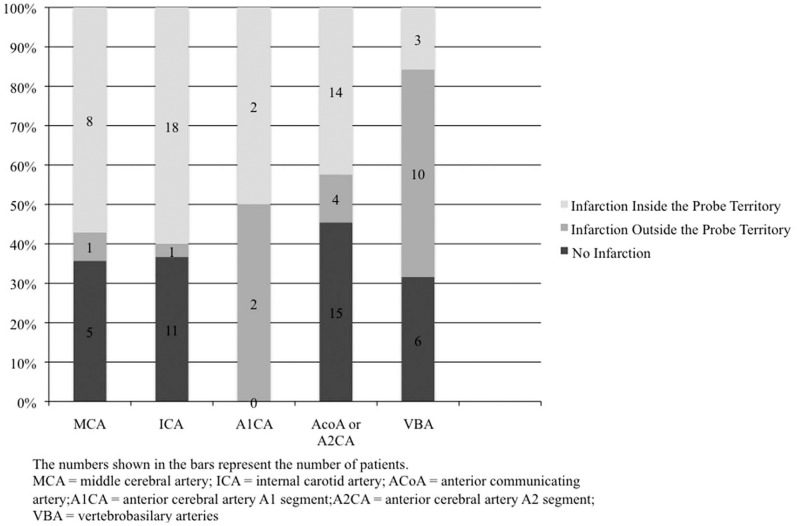
Results: We analyzed 100 patients after SAH caused by aneurysms located in the following locations: MCA (n = 14), ICA (n = 30), A1CA (n = 4), AcoA or A2CA (n = 33), and VBA (n = 19). Sensor location corresponded with CVS territory in 93% of MCA, 87% of ICA, 76% of AcoA or A2CA, but only 50% of A1CA and 42% of VBA aneurysms. The focal probe was located inside the infarction territory in 95% of ICA, 89% of MCA, 78% of ACoA or A2CA, 50% of A1CA and 23% of VBA aneurysms.
Conclusion: The probability that a single focal probe will be situated in the territory of severe CVS and infarction varies. It seems to be reasonably accurate for MCA and ICA aneurysms, but not for ACA or VBA aneurysms.
Conflict of interest statement
Figures
References
-
- van Gijn J, Kerr RS, Rinkel GJ (2007) Subarachnoid haemorrhage. Lancet 369: 306–318. - PubMed
-
- Sarrafzadeh A, Haux D, Sakowitz O, Benndorf G, Herzog H, et al. (2003) Acute focal neurological deficits in aneurysmal subarachnoid hemorrhage: relation of clinical course, CT findings, and metabolite abnormalities monitored with bedside microdialysis. Stroke 34: 1382–1388. - PubMed
-
- Charpentier C, Audibert G, Guillemin F, Civit T, Ducrocq X, et al. (1999) Multivariate analysis of predictors of cerebral vasospasm occurrence after aneurysmal subarachnoid hemorrhage. Stroke 30: 1402–1408. - PubMed
-
- Rabinstein AA, Friedman JA, Weigand SD, McClelland RL, Fulgham JR, et al. (2004) Predictors of cerebral infarction in aneurysmal subarachnoid hemorrhage. Stroke 35: 1862–1866. - PubMed
-
- Suarez JI, Qureshi AI, Yahia AB, Parekh PD, Tamargo RJ, et al. (2002) Symptomatic vasospasm diagnosis after subarachnoid hemorrhage: evaluation of transcranial Doppler ultrasound and cerebral angiography as related to compromised vascular distribution. Crit Care Med 30: 1348–1355. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
