

Imported human rabies cases worldwide, 1990-2012
- PMID: 23658853
- PMCID: PMC3642086
- DOI: 10.1371/journal.pntd.0002209
Imported human rabies cases worldwide, 1990-2012
Abstract
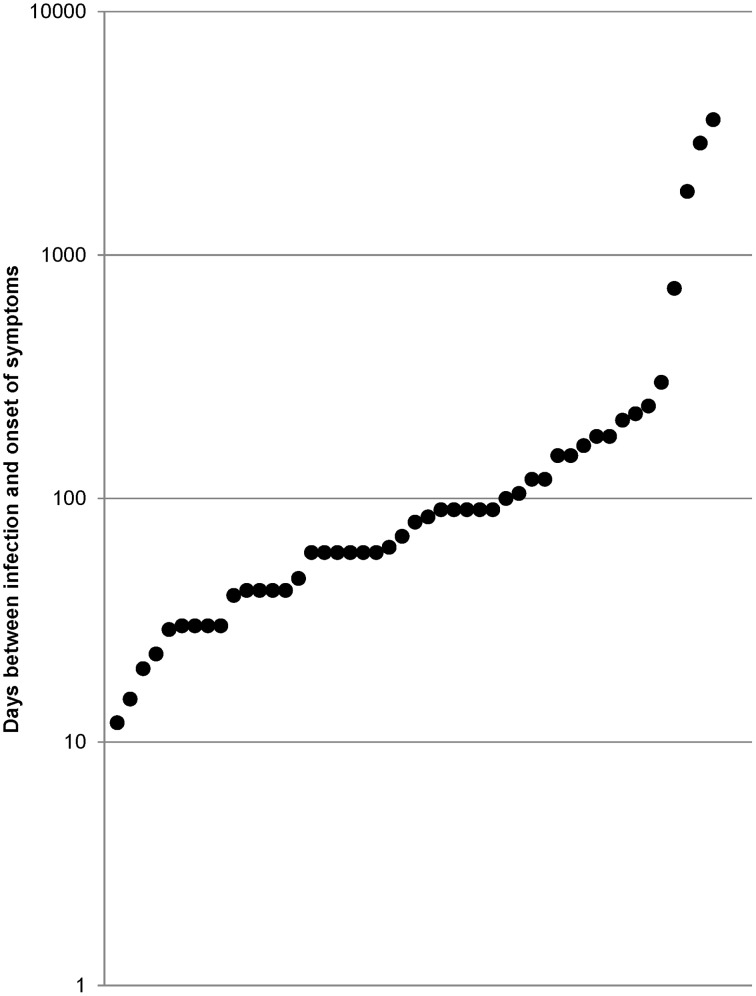
Sixty cases of human rabies in international travelers were reviewed from 1990-2012. A significant proportion of the cases were observed in migrants or their descendants when emigrating from their country of origin or after a trip to visit friends and relatives or for other reasons (43.3%). The cases were not necessarily associated with long-term travel or expatriation to endemic countries; moreover, cases were observed in travelers after short trips of two weeks or less. A predominance of male patients was observed (75.0%). The proportion of children was low (11.7%). Cases from India and Philippines were frequent (16 cases/60). In a significant proportion of cases (51.1%), diagnosis was challenging, with multiple missed diagnoses and transfers from ward to ward before the final diagnosis of rabies. Among the 28 patients whose confirmed diagnosis was obtained ante-mortem, the mean time between hospitalization and diagnosis was 7.7 days (median time: 6.0 days, range 2-30) including four cases with a diagnosis delayed by 15 or more days. In five cases, a patient traveled through one or more countries before ultimately being hospitalized. Three factors played a role in delaying the diagnosis of rabies in a number of cases: (i) a low index of suspicion for rabies in countries where the disease has been eradicated for a long time or is now rare, (ii) a negative history of animal bites or exposure to rabies, and (iii) atypical clinical presentation of the disease. Clinical symptomatology of rabies is complex and commonly confuses physicians. Furthermore, failure in diagnosing imported cases in more developed countries is most likely related to the lack of medical familiarity with even the typical clinical features of the disease.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


Comment in
-
Human rabies, a disease of the poor - also in travelers?Pathog Glob Health. 2013 Oct;107(7):338-9. doi: 10.1179/2047772413Z.000000000167. Pathog Glob Health. 2013. PMID: 24392675 Free PMC article. No abstract available.
Similar articles
-
Epidemiology of rabies cases among international travellers, 2013-2019: A retrospective analysis of published reports.Travel Med Infect Dis. 2020 Jul-Aug;36:101766. doi: 10.1016/j.tmaid.2020.101766. Epub 2020 Jun 7. Travel Med Infect Dis. 2020. PMID: 32525075
-
Animal-associated exposure to rabies virus among travelers, 1997-2012.Emerg Infect Dis. 2015 Apr;21(4):569-77. doi: 10.3201/eid2104.141479. Emerg Infect Dis. 2015. PMID: 25811076 Free PMC article.
-
Rabies exposure in international travelers: do we miss the target?Int J Infect Dis. 2010 Mar;14(3):e243-6. doi: 10.1016/j.ijid.2009.05.009. Epub 2009 Aug 12. Int J Infect Dis. 2010. PMID: 19674923
-
Assessment of rabies exposure risk among Israeli travelers.Travel Med Infect Dis. 2008 Jan-Mar;6(1-2):12-6. doi: 10.1016/j.tmaid.2007.09.041. Epub 2007 Oct 25. Travel Med Infect Dis. 2008. PMID: 18342268
-
Rabies pretravel vaccination.Curr Opin Infect Dis. 2012 Oct;25(5):500-6. doi: 10.1097/QCO.0b013e3283567b35. Curr Opin Infect Dis. 2012. PMID: 22825289 Review.
Cited by
-
Traveller exposures to animals: a GeoSentinel analysis.J Travel Med. 2020 Nov 9;27(7):taaa010. doi: 10.1093/jtm/taaa010. J Travel Med. 2020. PMID: 31993666 Free PMC article.
-
Pre-exposure rabies vaccination among US international travelers: findings from the global TravEpiNet consortium.Vector Borne Zoonotic Dis. 2014 Feb;14(2):160-7. doi: 10.1089/vbz.2013.1381. Epub 2013 Dec 20. Vector Borne Zoonotic Dis. 2014. PMID: 24359420 Free PMC article.
-
Perceptions and Practices of Mass Bat Exposure Events in the Setting of Rabies Among U.S. Public Health Agencies.Zoonoses Public Health. 2017 Mar;64(2):127-136. doi: 10.1111/zph.12289. Epub 2016 Jul 8. Zoonoses Public Health. 2017. PMID: 27389926 Free PMC article.
-
Epidemiology, transmission dynamics, risk factors, and future directions of rabies in the Arabian Peninsula using one health approach: a review.Eur J Public Health. 2025 Jan 1;35(Supplement_1):i14-i22. doi: 10.1093/eurpub/ckae164. Eur J Public Health. 2025. PMID: 39801328 Free PMC article.
-
An Overview of the Most Significant Zoonotic Viral Pathogens Transmitted from Animal to Human in Saudi Arabia.Pathogens. 2019 Feb 22;8(1):25. doi: 10.3390/pathogens8010025. Pathogens. 2019. PMID: 30813309 Free PMC article. Review.
References
-
- Gautret P, Parola P (2012) Rabies vaccination for international travelers. Vaccine 30: 126–133. - PubMed
-
- Malerczyk C, Detora L, Gniel D (2011) Imported human rabies cases in Europe, the United States, and Japan, 1990 to 2010. J Travel Med 18: 402–7. - PubMed
-
- van Thiel PP, van den Hoek JAR, Eftimov F, Tepaske R, Zaaijer HJ, et al. (2007) Fatal case of human rabies (Duvenhage virus) from a bat in Kenya: the Netherlands, December 2007. Rabies Bulletin Europe 31: 5–6. - PubMed
-
- van Thiel PP, van den Hoek JA, Eftimov F, Tepaske R, Zaaijer HJ, et al. (2008) Fatal case of human rabies (Duvenhage virus) from a bat in Kenya: the Netherlands, December 2007. Euro Surveill 13: e428. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
