

Tentorial dural fistulas: endovascular management and description of the medial dural-tentorial branch of the superior cerebellar artery
- PMID: 23660293
- PMCID: PMC7965633
- DOI: 10.3174/ajnr.A3519
Tentorial dural fistulas: endovascular management and description of the medial dural-tentorial branch of the superior cerebellar artery
Abstract
Background and purpose: TDAVFs are uncommon causes of spontaneous intracranial hemorrhage. A retrospective review of their management was performed after repeatedly observing a previously under-recognized medial dural-tentorial branch of the SCA.
Materials and methods: Thirteen patients were diagnosed with TDAVFs by CT/MR imaging and DSA during a 5.8-year period. Seven patients presented after intracranial hemorrhage. Twelve patients were treated endovascularly, and one, surgically.
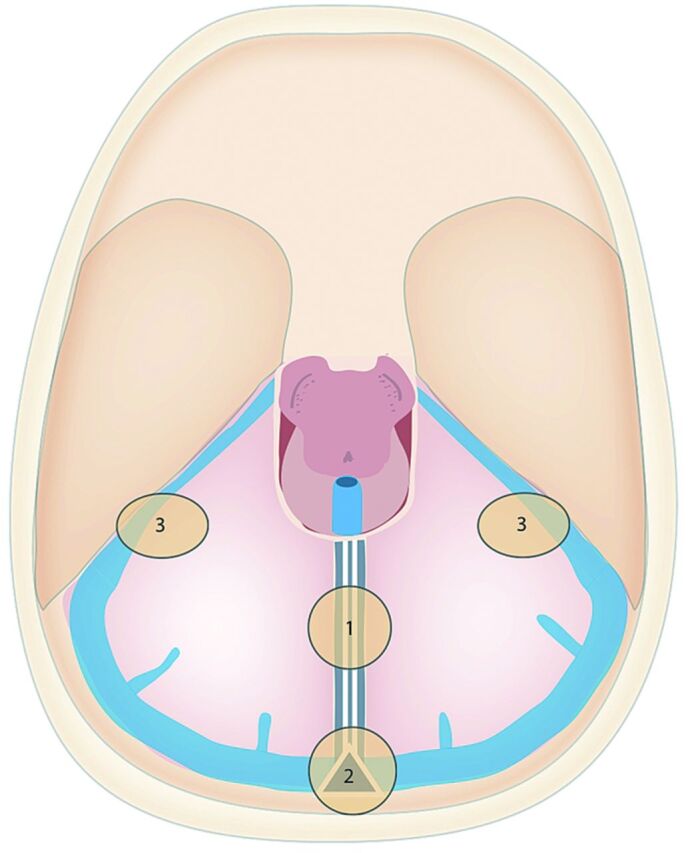
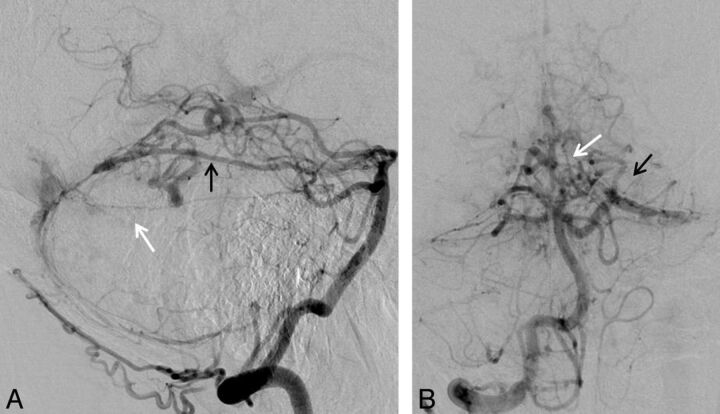
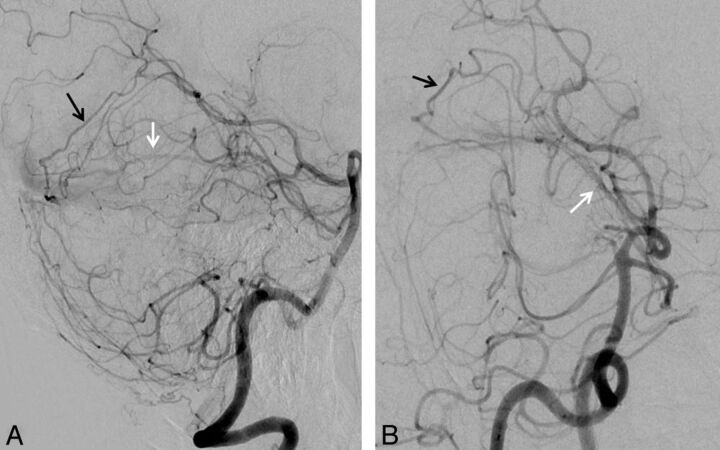
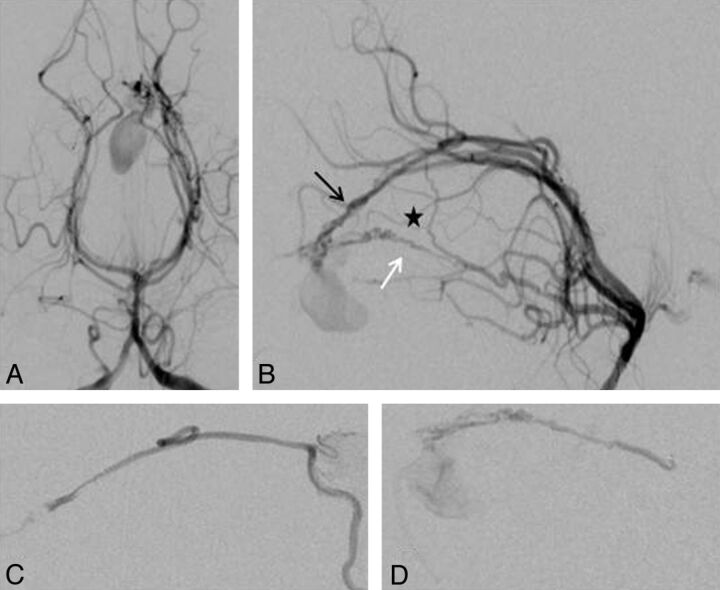
Results: Eleven TDAVFs were located in the midline (7 at the falx cerebelli and 4 at the torcular), and 2 were petrotentorial. All torcular TDAVFs were associated with sinus thrombosis and showed bidirectional drainage relative to the tentorium. No sinus thrombosis was seen in the falx cerebelli subtype, which drained infratentorially only, except in 1 patient who had had unrelated surgery previously. Venous drainage was directly to cortical veins except for 1 petrotentorial and 2 torcular TDAVFs. A branch of the SCA, the medial dural-tentorial artery, was observed in 5 midline TDAVFs. Its anatomy was defined with selective angiography. Endovascular therapy resulted in a cure in 5 and subtotal occlusion in 6, and staged treatment is ongoing in 1 patient. One patient was cured after surgery.
Conclusions: TDAVFs frequently cause intracranial hemorrhage and therefore warrant treatment. Endovascular therapy proved effective in this series, and arteriography was essential for understanding the various fistula subtypes and for treatment planning. We emphasize the importance of recognizing the medial dural-tentorial artery of the SCA with its characteristic course along the tentorium on angiography. This artery should be included in future anatomic descriptions of the cranial blood supply.
Figures
References
-
- Kajita Y, Miyachi S, Wakabayashi T, et al. A dural arteriovenous fistula of the tentorium successfully treated by intravascular embolization. Surg Neurol 1999;52:294–98 - PubMed
-
- Zhou LF, Chen L, Song DL, et al. Tentorial dural arteriovenous fistulas. Surg Neurol 2007;67:472–81 - PubMed
-
- van Lindert E, Hassler W, Kühne D, et al. Combined endovascular-microsurgical treatment of tentorial-incisural dural arteriovenous malformations: report of five cases. Minim Invasive Neurosurg 2000;43:138–43 - PubMed
-
- Picard L, Bracard S, Islak C, et al. Dural fistulae of the tentorium cerebelli: radioanatomical, clinical and therapeutic considerations. J Neuroradiol 1990;17:161–81 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources