

Energy loss and coronary flow simulation following hybrid stage I palliation: a hypoplastic left heart computational fluid dynamic model
- PMID: 23660734
- PMCID: PMC3715191
- DOI: 10.1093/icvts/ivt193
Energy loss and coronary flow simulation following hybrid stage I palliation: a hypoplastic left heart computational fluid dynamic model
Abstract
Objectives: The theoretical differences in energy losses as well as coronary flow with different band sizes for branch pulmonary arteries (PA) in hypoplastic left heart syndrome (HLHS) remain unknown. Our objective was to develop a computational fluid dynamic model (CFD) to determine the energy losses and pulmonary-to-systemic flow rates. This study was done for three different PA band sizes.
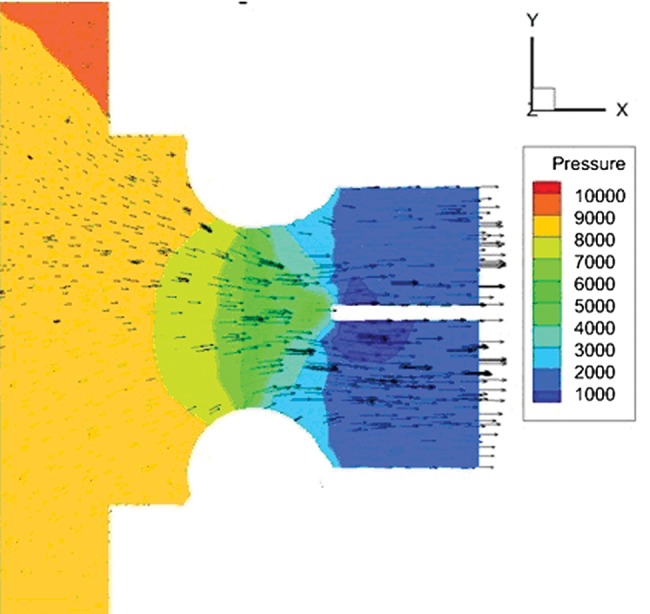
Methods: Three-dimensional computer models of the hybrid procedure were constructed using the standard commercial CFD softwares Fluent and Gambit. The computer models were controlled for bilateral PA reduction to 25% (restrictive), 50% (intermediate) and 75% (loose) of the native branch pulmonary artery diameter. Velocity and pressure data were calculated throughout the heart geometry using the finite volume numerical method. Coronary flow was measured simultaneously with each model. Wall shear stress and the ratio of pulmonary-to-systemic volume flow rates were calculated. Computer simulations were compared at fixed points utilizing echocardiographic and catheter-based metric dimensions.
Results: Restricting the PA band to a 25% diameter demonstrated the greatest energy loss. The 25% banding model produced an energy loss of 16.76% systolic and 24.91% diastolic vs loose banding at 7.36% systolic and 17.90% diastolic. Also, restrictive PA bands had greater coronary flow compared with loose PA bands (50.2 vs 41.9 ml/min). Shear stress ranged from 3.75 Pascals with restrictive PA banding to 2.84 Pascals with loose banding. Intermediate PA banding at 50% diameter achieved a Qp/Qs (closest to 1) at 1.46 systolic and 0.66 diastolic compared with loose or restrictive banding without excess energy loss.
Conclusions: CFD provides a unique platform to simulate pressure, shear stress as well as energy losses of the hybrid procedure. PA banding at 50% provided a balanced pulmonary and systemic circulation with adequate coronary flow but without extra energy losses incurred.
Keywords: Computational fluid dynamics; Haemodynamics; Hypoplastic left heart syndrome; Navier–Stokes equations; Simulations.
Figures



Similar articles
-
Effects of pulmonary artery banding and retrograde aortic arch obstruction on the hybrid palliation of hypoplastic left heart syndrome.J Thorac Cardiovasc Surg. 2013 Dec;146(6):1341-8. doi: 10.1016/j.jtcvs.2013.01.038. Epub 2013 Feb 20. J Thorac Cardiovasc Surg. 2013. PMID: 23434295
-
Surgical Modulation of Pulmonary Artery Shear Stress: A Patient-Specific CFD Analysis of the Norwood Procedure.Cardiovasc Eng Technol. 2024 Aug;15(4):431-442. doi: 10.1007/s13239-024-00724-3. Epub 2024 Mar 8. Cardiovasc Eng Technol. 2024. PMID: 38459240 Free PMC article.
-
Norwood with right ventricle-to-pulmonary artery conduit is more effective than Norwood with Blalock-Taussig shunt for hypoplastic left heart syndrome: mathematic modeling of hemodynamics.Eur J Cardiothorac Surg. 2011 Dec;40(6):1412-7; discussion 1417-8. doi: 10.1016/j.ejcts.2011.03.033. Epub 2011 May 5. Eur J Cardiothorac Surg. 2011. PMID: 21546259
-
Does bilateral pulmonary banding in comparison to Norwood procedure improve outcome in neonates with hypoplastic left heart syndrome beyond second-stage palliation? A review of the current literature.Thorac Cardiovasc Surg. 2012 Apr;60(3):181-8. doi: 10.1055/s-0031-1295569. Epub 2012 Jan 3. Thorac Cardiovasc Surg. 2012. PMID: 22215495 Review.
-
Giessen Procedure as Comprehensive Stage II Palliation With Aortic Arch Reconstruction After Hybrid Bilateral Pulmonary Artery Banding and Ductal Stenting for Hypoplastic Left Heart Syndrome.Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2018 Mar;21:19-27. doi: 10.1053/j.pcsu.2017.11.007. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2018. PMID: 29425520 Review.
Cited by
-
Application of physics-based flow models in cardiovascular medicine: Current practices and challenges.Biophys Rev (Melville). 2021 Mar 22;2(1):011302. doi: 10.1063/5.0040315. eCollection 2021 Mar. Biophys Rev (Melville). 2021. PMID: 38505399 Free PMC article. Review.
References
-
- Norwood WI, Lang P, Castaneda AR, Campbell DN. Experience with operations for hypoplastic left heart syndrome. J Thorac Cardiovasc Surg. 1981;85:511–9. - PubMed
-
- Ohye RG, Sleeper LA, Mahony L, Newburger JW, Pearson GD, Lu M Pediatric Heart Network Investigators. Comparison of shunt types in the Norwood procedure for single-ventricle lesions. N Engl J Med. 2010;362:1980–92. doi:10.1056/NEJMoa0912461. - DOI - PMC - PubMed
-
- Galantowicz M, Cheatham JP, Phillips A, Cua CL, Hoffman TM, Hill SL, et al. Hybrid approach for hypoplastic left heart syndrome: intermediate results after the learning curve. Ann Thorac Surg. 2008;85:2063–70. discussion 2070–1 doi:10.1016/j.athoracsur.2008.02.009. - DOI - PubMed
-
- Pigula FA, Vida V, Del Nido P, Bacha E. Contemporary results and current strategies in the management of hypoplastic left heart syndrome. Semin Thorac Cardiovasc Surg. 2007;19:238–44. doi:10.1053/j.semtcvs.2007.07.002. - DOI - PubMed
-
- De Leval MR, Kilner P, Gewillig M, Bull C. Total cavopulmonary connection: a logical alternative to atriopulmonary connection for complex Fontan operations. J Thorac Cardiovasc Surg. 1988;96:682–95. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
