

Model-based patterns in prostate cancer mortality worldwide
- PMID: 23660943
- PMCID: PMC3681014
- DOI: 10.1038/bjc.2013.217
Model-based patterns in prostate cancer mortality worldwide
Abstract
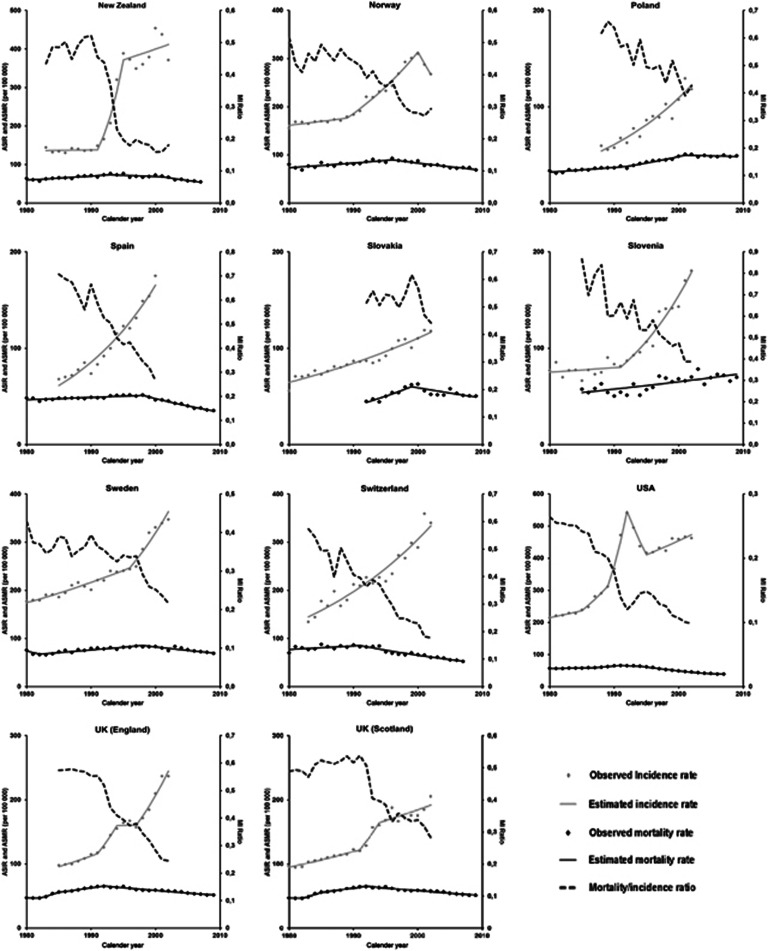
Background: Prostate cancer mortality has been decreasing in several high income countries and previous studies analysed the trends mostly according to geographical criteria. We aimed to identify patterns in the time trends of prostate cancer mortality across countries using a model-based approach.
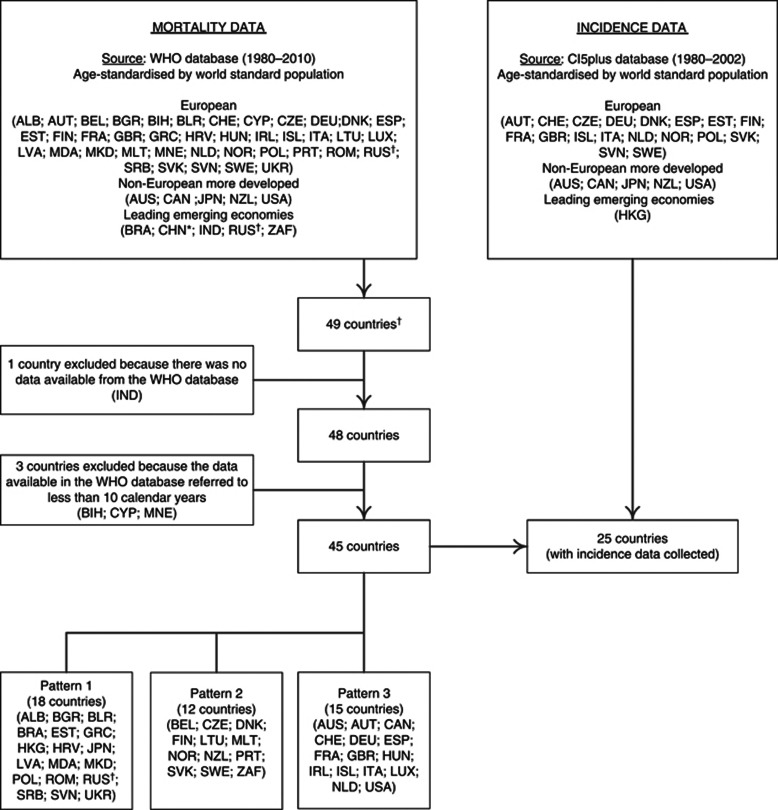
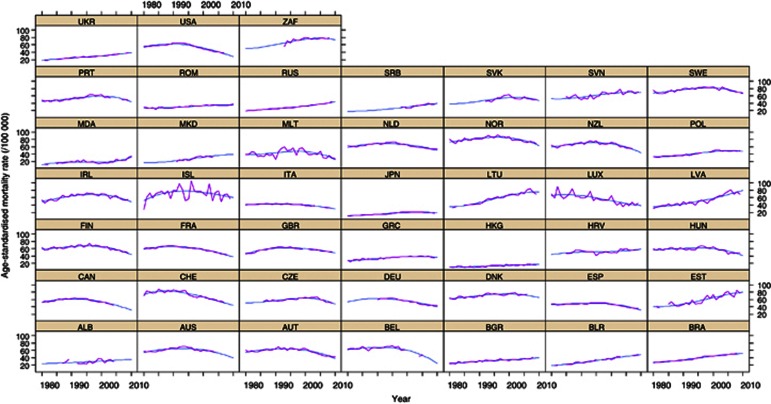
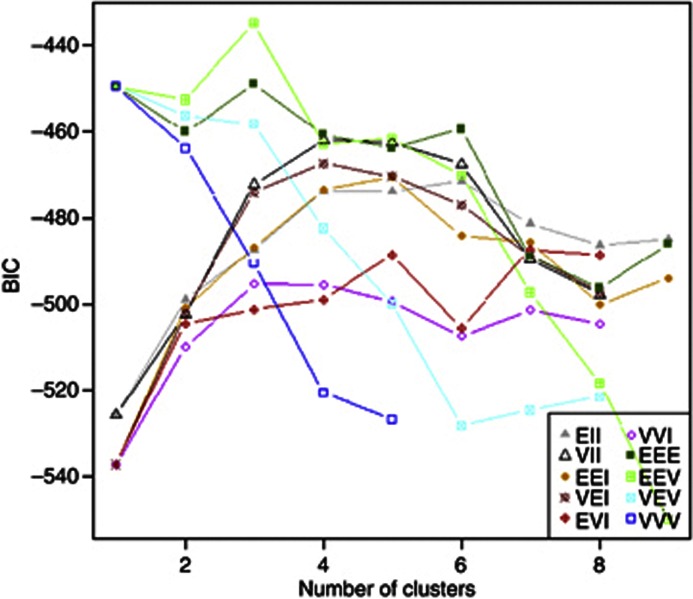
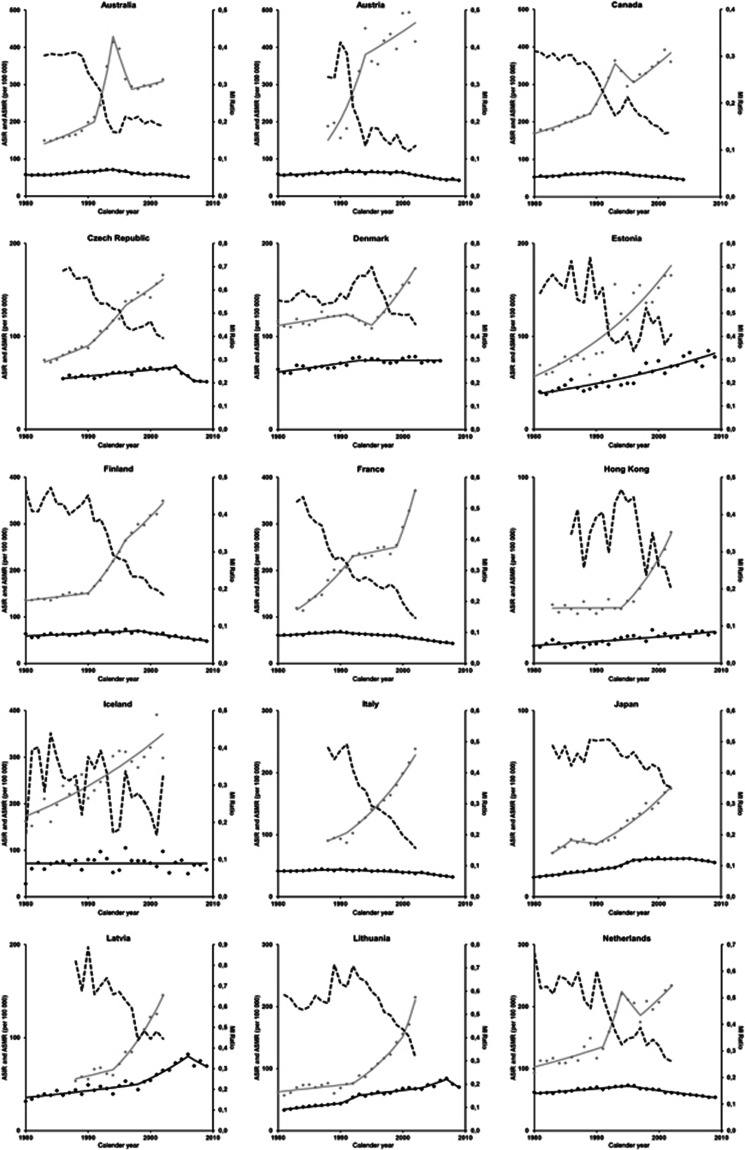
Methods: Model-based clustering was used to identify patterns of variation in prostate cancer mortality (1980-2010) across 37 European, five non-European high-income countries and four leading emerging economies. We characterised the patterns observed regarding the geographical distribution and gross national income of the countries, as well as the trends observed in mortality/incidence ratios.
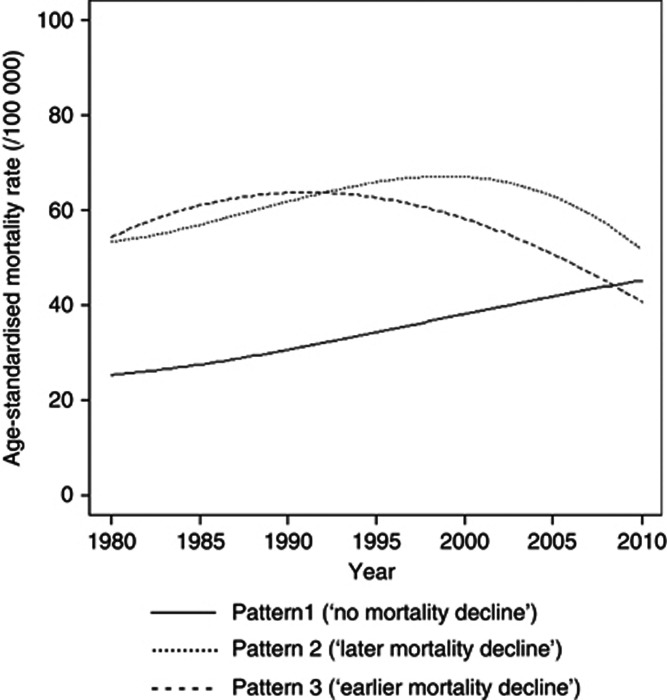
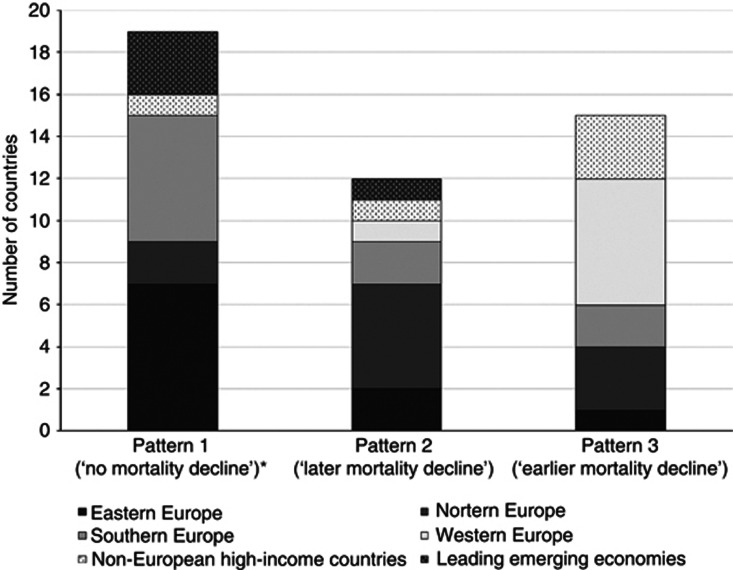
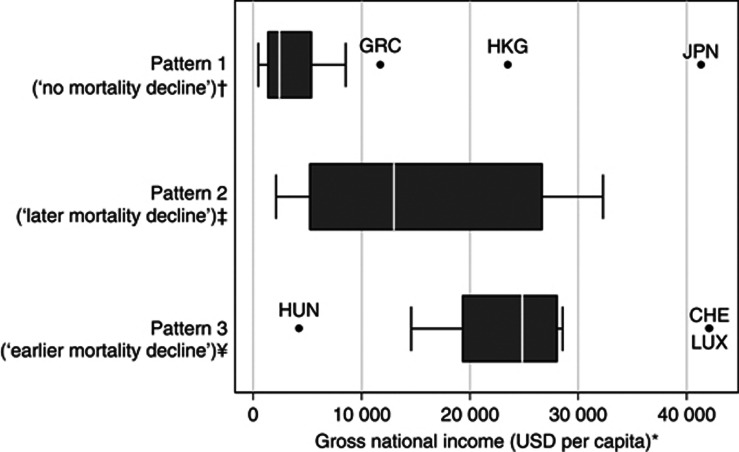
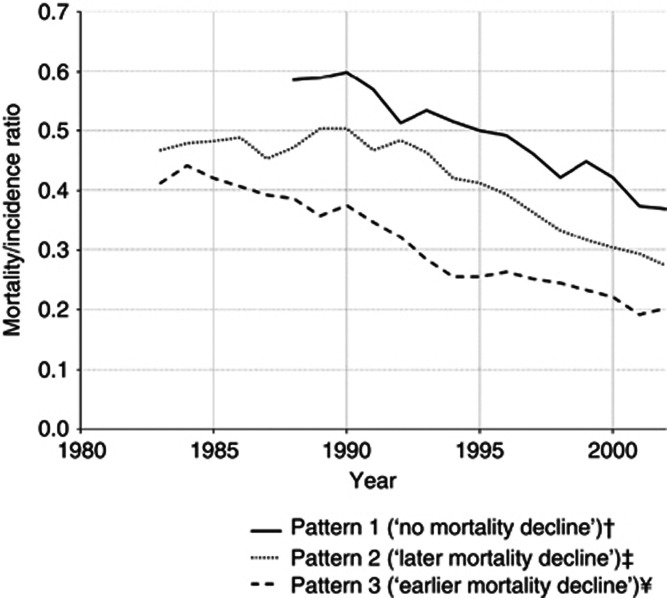
Results: We identified three clusters of countries with similar variation in prostate cancer mortality: pattern 1 ('no mortality decline'), characterised by a continued increase throughout the whole period; patterns 2 ('later mortality decline') and 3 ('earlier mortality decline') depict mortality declines, starting in the late and early 1990s, respectively. These clusters are also homogeneous regarding the variation in the prostate cancer mortality/incidence ratios, while are heterogeneous with reference to the geographical region of the countries and distribution of the gross national income.
Conclusion: We provide a general model for the description and interpretation of the trends in prostate cancer mortality worldwide, based on three main patterns.
Figures
References
-
- Andriole GL, Crawford ED, Grubb RLr, Buys SS, Chia D, Church TR, Fouad MN, Isaacs C, Kvale P, Reding DJ, Weissfeld JL, Yokochi LA, O'Brien B, Ragard LR, Clapp JD, Rathmell JM, Riley TL, Hsing AW, Izmirlian G, Pinsky PF, Kramer BS, Miller AB, Gohagan JK, Prorok PC. Prostate cancer screening in the randomized prostate, lung, colorectal, and ovarian cancer screening trial: mortality results after 13 years of follow-up. J Natl Cancer Inst. 2012;104 (2:125–132. - PMC - PubMed
-
- Bill-Axelson A, Holmberg L, Ruutu M, Garmo H, Stark JR, Busch C, Nordling S, Häggman M, Andersson SO, Bratell S, Spångberg A, Palmgren J, Steineck G, Adami HO, Johansson J. Radical prostatectomy versus watchful waiting in early prostate cancer. N Engl J Med. 2011;364 (48:1708–1717. - PubMed
-
- Bolla M, Collette L, Blank L, Warde P, Dubois JB, Mirimanoff RO, Storme G, Bernier J, Kuten A, Sternberg C, Mattelaer J, Lopez Torecilla J, Pfeffer JR, Lino Cutajar C, Zurlo A, Pierart M. Long-term results with immediate androgen suppression and external irradiation in patients with locally advanced prostate cancer (an EORTC study): a phase III randomised trial. Lancet. 2002;360 (9327:103–106. - PubMed
-
- Bosetti C, Bertuccio P, Chatenoud L, Negri E, La Vecchia C, Levi F. Trends in mortality from urologic cancers in Europe, 1970–2008. Eur Urol. 2011;60 (1:1–15. - PubMed
-
- Bouchardy C, Fioretta G, Rapiti E, Verkooijen HM, Rapin CH, Schmidlin F, Miralbell R, Zanetti R. Recent trends in prostate cancer mortality show a continuos decrease in several countries. Int J Cancer. 2008;123 (2:421–429. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
