

Herbal therapies for type 2 diabetes mellitus: chemistry, biology, and potential application of selected plants and compounds
- PMID: 23662132
- PMCID: PMC3638592
- DOI: 10.1155/2013/378657
Herbal therapies for type 2 diabetes mellitus: chemistry, biology, and potential application of selected plants and compounds
Abstract
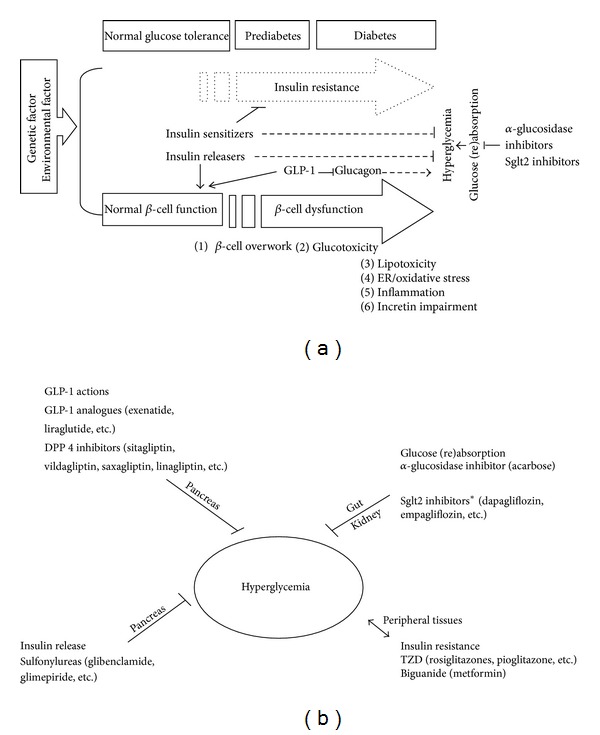
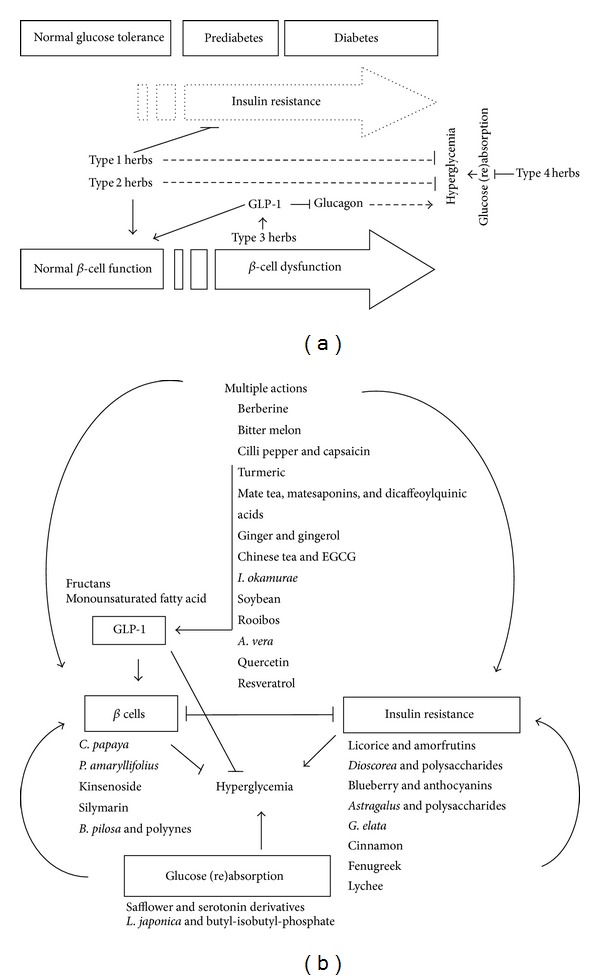
Diabetes mellitus has been recognized since antiquity. It currently affects as many as 285 million people worldwide and results in heavy personal and national economic burdens. Considerable progress has been made in orthodox antidiabetic drugs. However, new remedies are still in great demand because of the limited efficacy and undesirable side effects of current orthodox drugs. Nature is an extraordinary source of antidiabetic medicines. To date, more than 1200 flowering plants have been claimed to have antidiabetic properties. Among them, one-third have been scientifically studied and documented in around 460 publications. In this review, we select and discuss blood glucose-lowering medicinal herbs that have the ability to modulate one or more of the pathways that regulate insulin resistance, β-cell function, GLP-1 homeostasis, and glucose (re)absorption. Emphasis is placed on phytochemistry, anti-diabetic bioactivities, and likely mechanism(s). Recent progress in the understanding of the biological actions, mechanisms, and therapeutic potential of compounds and extracts of plant origin in type 2 diabetes is summarized. This review provides a source of up-to-date information for further basic and clinical research into herbal therapy for type 2 diabetes. Emerging views on therapeutic strategies for type 2 diabetes are also discussed.
Figures
References
-
- Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Research and Clinical Practice. 2010;87(1):4–14. - PubMed
-
- Boyle JP, Engelgau MM, Thompson TJ, et al. Estimating prevalence of type 1 and type 2 diabetes in a population of African Americans with diabetes mellitus. American Journal of Epidemiology. 1999;149(1):55–63. - PubMed
-
- Attele AS, Zhou YP, Xie JT, et al. Antidiabetic effects of Panax ginseng berry extract and the identification of an effective component. Diabetes. 2002;51(6):1851–1858. - PubMed
-
- Cashen A, Lopez S, Gao F, et al. A phase II Study of plerixafor (AMD3100) plus G-CSF for autologous hematopoietic progenitor cell mobilization in patients with hodgkin lymphoma. Biology of Blood and Marrow Transplantation. 2008;14(11):1253–1261. - PubMed
-
- Laakso M. Insulin resistance and its impact on the approach to therapy of Type 2 diabetes. International Journal of Clinical Practice, Supplement. 2001;(121):8–12. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
