

Metabolism and bioenergetics in the right ventricle and pulmonary vasculature in pulmonary hypertension
- PMID: 23662191
- PMCID: PMC3641722
- DOI: 10.4103/2045-8932.109960
Metabolism and bioenergetics in the right ventricle and pulmonary vasculature in pulmonary hypertension
Abstract
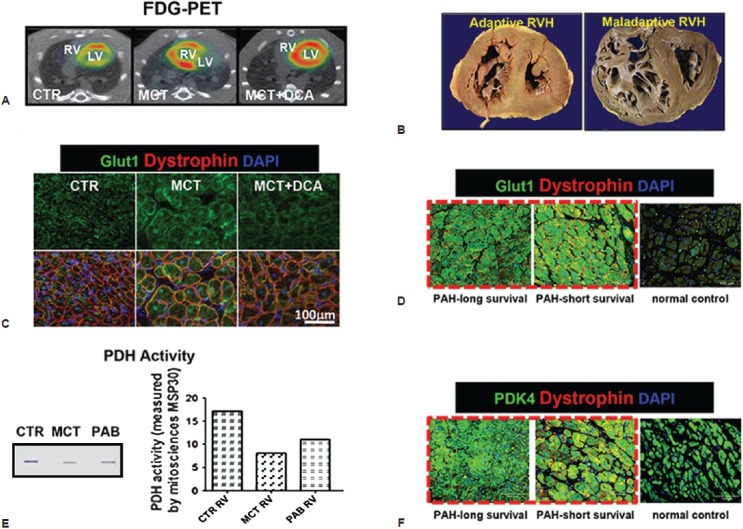
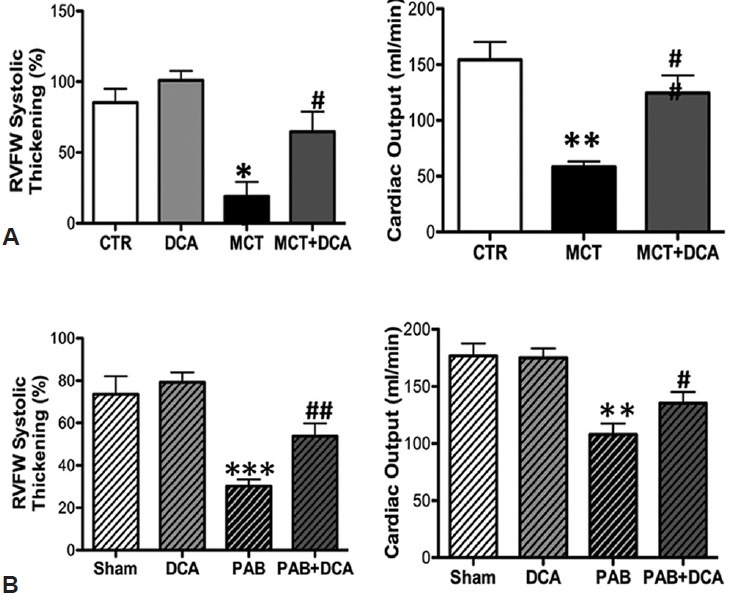
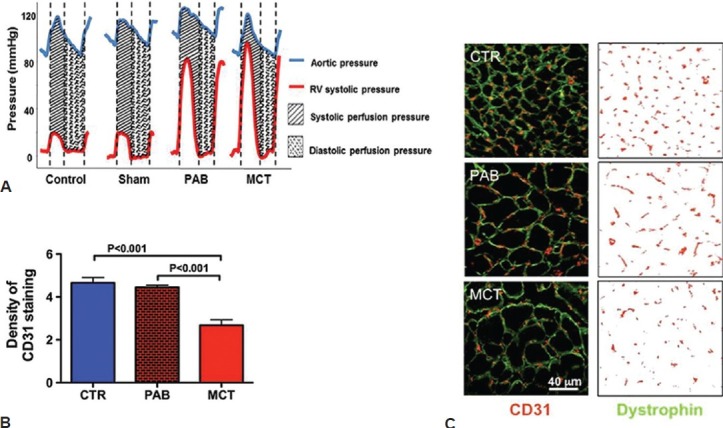
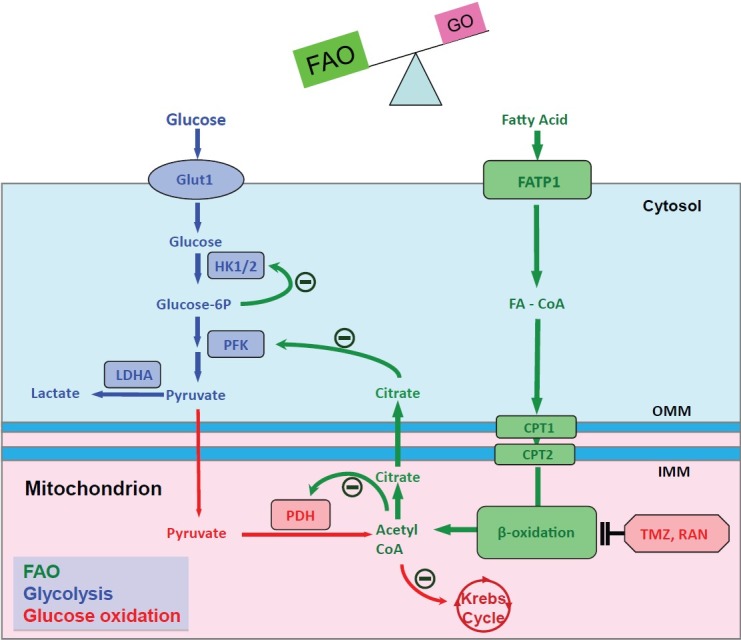
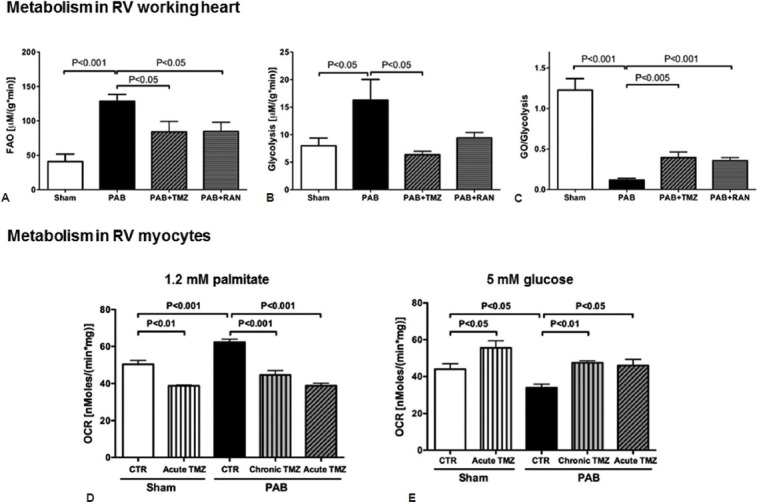
Pulmonary arterial hypertension (PAH) is a syndrome in which pulmonary vascular cross sectional area and compliance are reduced by vasoconstriction, vascular remodeling, and inflammation. Vascular remodeling results in part from increased proliferation and impaired apoptosis of vascular cells. The resulting increase in afterload promotes right ventricular hypertrophy (RVH) and RV failure. Recently identified mitochondrial-metabolic abnormalities in PAH, notably pyruvate dehydrogenase kinase-mediated inhibition of pyruvate dehydrogenase (PDH), result in aerobic glycolysis in both the lung vasculature and RV. This glycolytic shift has diagnostic importance since it is detectable early in experimental PAH by increased lung and RV uptake of (18)F-fluorodeoxyglucose on positron emission tomography. The metabolic shift also has pathophysiologic and therapeutic relevance. In RV myocytes, the glycolytic switch reduces contractility while in the vasculature it renders cells hyperproliferative and apoptosis-resistant. Reactivation of PDH can be achieved directly by PDK inhibition (using dichloroacetate), or indirectly via activating the Randle cycle, using inhibitors of fatty acid oxidation (FAO), trimetazidine and ranolazine. In experimental PAH and RVH, PDK inhibition increases glucose oxidation, enhances RV function, regresses pulmonary vascular disease by reducing proliferation and enhancing apoptosis, and restores cardiac repolarization. FAO inhibition increases RV glucose oxidation and RV function in experimental RVH. The trigger for metabolic remodeling in the RV and lung differ. In the RV, metabolic remodeling is likely triggered by ischemia (due to microvascular rarefaction and/or reduced coronary perfusion pressure). In the vasculature, metabolic changes result from redox-mediated activation of transcription factors, including hypoxia-inducible factor 1α, as a consequence of epigenetic silencing of SOD2 and/or changes in mitochondrial fission/fusion. Randomized controlled trials are required to assess whether the benefits of enhancing glucose oxidation are realized in patients with PAH.
Keywords: aerobic glycolysis; fatty acid oxidation; pyruvate dehydrogenase kinase; right ventricular ischemia; the Randle cycle.
Conflict of interest statement
Figures
References
-
- Simonneau G, Robbins IM, Beghetti M, Channick RN, Delcroix M, Denton CP, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2009;54:S43–54. - PubMed
-
- Vlahakes GJ, Turley K, Hoffman JI. The pathophysiology of failure in acute right ventricular hypertension: Hemodynamic and biochemical correlations. Circulation. 1981;63:87–95. - PubMed
-
- Bogaard HJ, Natarajan R, Henderson SC, Long CS, Kraskauskas D, Smithson L, et al. Chronic pulmonary artery pressure elevation is insufficient to explain right heart failure. Circulation. 2009;120:1951–60. - PubMed
-
- Torbicki A, Kurzyna M, Kuca P, Fijalkowska A, Sikora J, Florczyk M, et al. Detectable serum cardiac troponin t as a marker of poor prognosis among patients with chronic precapillary pulmonary hypertension. Circulation. 2003;108:844–8. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
