

Associations between the organisation of stroke services, process of care, and mortality in England: prospective cohort study
- PMID: 23667071
- PMCID: PMC3650920
- DOI: 10.1136/bmj.f2827
Associations between the organisation of stroke services, process of care, and mortality in England: prospective cohort study
Abstract
Objective: To estimate the relations between the organisation of stroke services, process measures of care quality, and 30 day mortality in patients admitted with acute ischaemic stroke.
Design: Prospective cohort study.
Setting: Hospitals (n=106) admitting patients with acute stroke in England and participating in the Stroke Improvement National Audit Programme and 2010 Sentinel Stroke Audit.
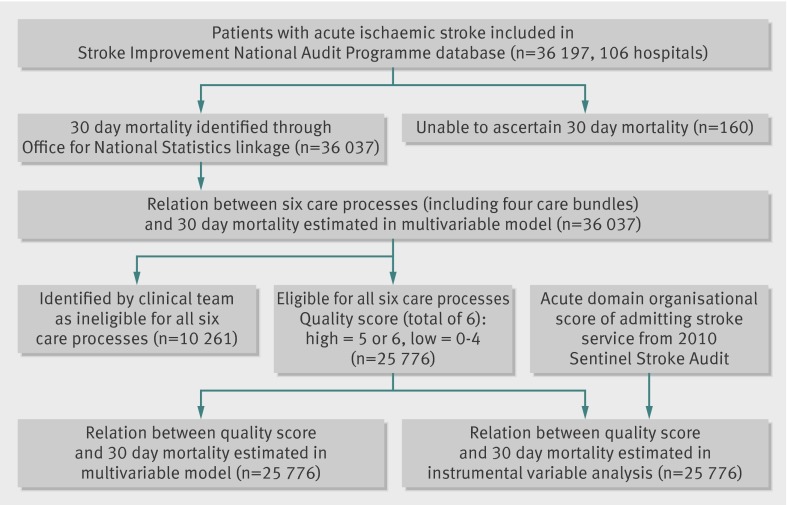
Participants: 36,197 adults admitted with acute ischaemic stroke to a participating hospital from 1 April 2010 to 30 November 2011.
Main outcome measure: Associations between process of care (the assessments, interventions, and treatments that patients receive) and 30 day all cause mortality, adjusting for patient level characteristics. Process of care was measured using six individual measures of stroke care and summarised into an overall quality score.
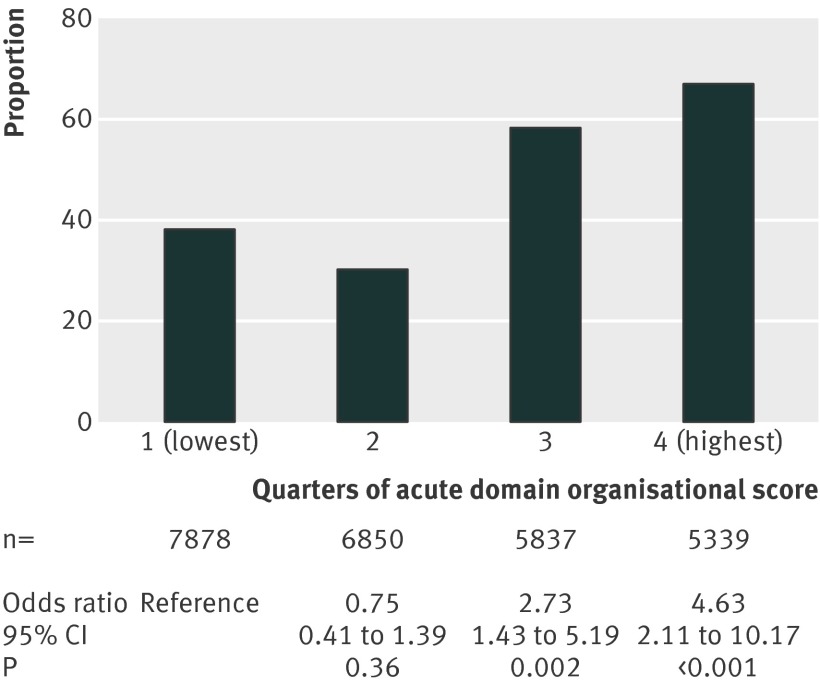
Results: Of 36,197 patients admitted with acute ischaemic stroke, 25,904 (71.6%) were eligible to receive all six care processes. Patients admitted to stroke services with high organisational scores were more likely to receive most (5 or 6) of the six care processes. Three of the individual processes were associated with reduced mortality, including two care bundles: review by a stroke consultant within 24 hours of admission (adjusted odds ratio 0.86, 95%confidence interval 0.78 to 0.96), nutrition screening and formal swallow assessment within 72 hours (0.83, 0.72 to 0.96), and antiplatelet therapy and adequate fluid and nutrition for first the 72 hours (0.55, 0.49 to 0.61). Receipt of five or six care processes was associated with lower mortality compared with receipt of 0-4 in both multilevel (0.74, 0.66 to 0.83) and instrumental variable analyses (0.62, 0.46 to 0.83).
Conclusions: Patients admitted to stroke services with higher levels of organisation are more likely to receive high quality care as measured by audited process measures of acute stroke care. Those patients receiving high quality care have a reduced risk of death in the 30 days after stroke, adjusting for patient characteristics and controlling for selection bias.
Conflict of interest statement
Competing interests: AGR is National Clinical Director of Stroke, NHS England. All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- Department of Health: Progress in improving stroke care. National Audit Office, 2010.
-
- National Clinical Guideline for Stroke, 4th edn.Intercollegiate Stroke Working Party. Royal College of Physicians, 2012.
-
- Wardlaw JM, Murray V, Berge E, Del Zoppo G. Thrombolysis for acute ischaemic stroke. Stroke 2010;41:e445-6.
-
- Alteplase for treating acute ischaemic stroke (TA 264). National Institute for Health and Clinical Excellence, 2012.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous