

Malaria control and the intensity of Plasmodium falciparum transmission in Namibia 1969-1992
- PMID: 23667604
- PMCID: PMC3646760
- DOI: 10.1371/journal.pone.0063350
Malaria control and the intensity of Plasmodium falciparum transmission in Namibia 1969-1992
Abstract
Background: Historical evidence of the levels of intervention scale up and its relationships to changing malaria risks provides important contextual information for current ambitions to eliminate malaria in various regions of Africa today.
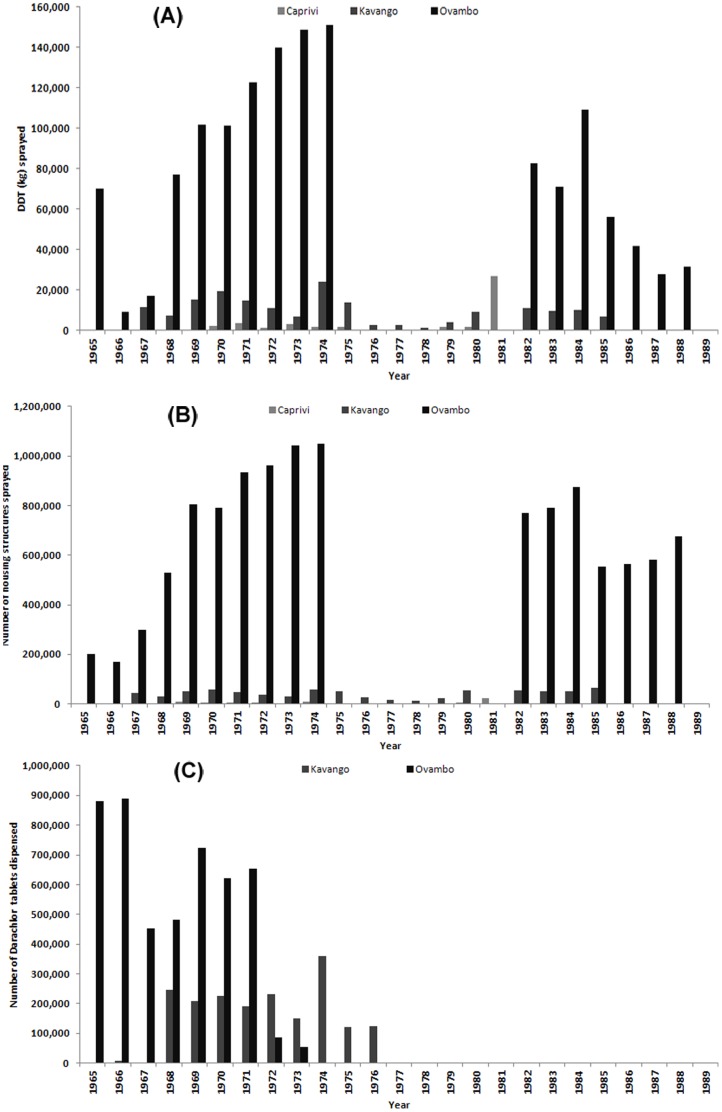
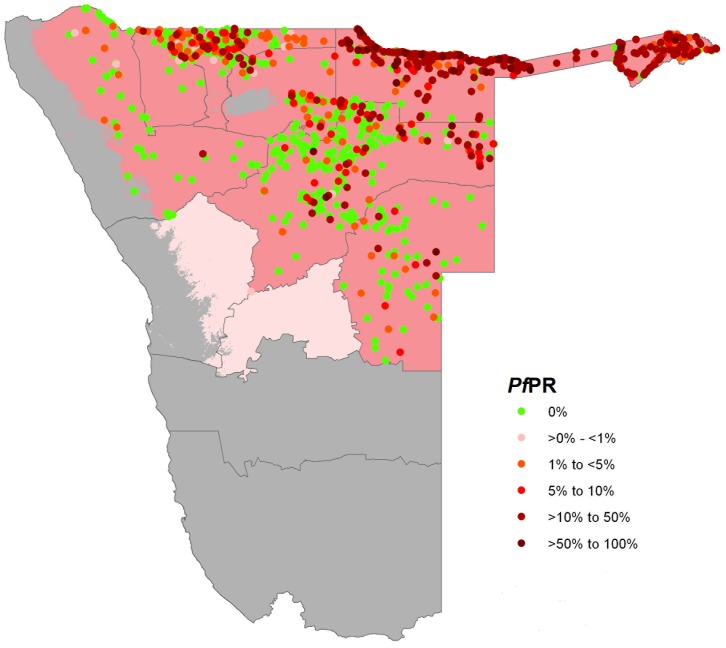
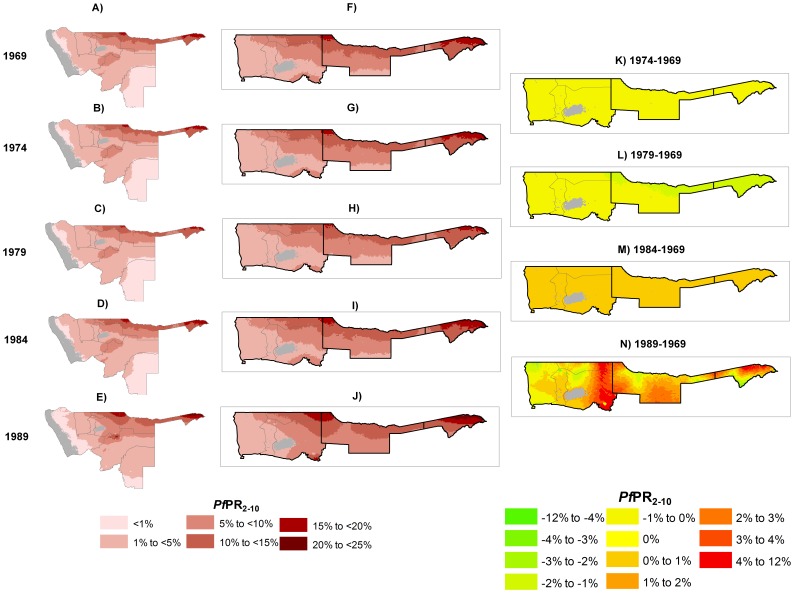
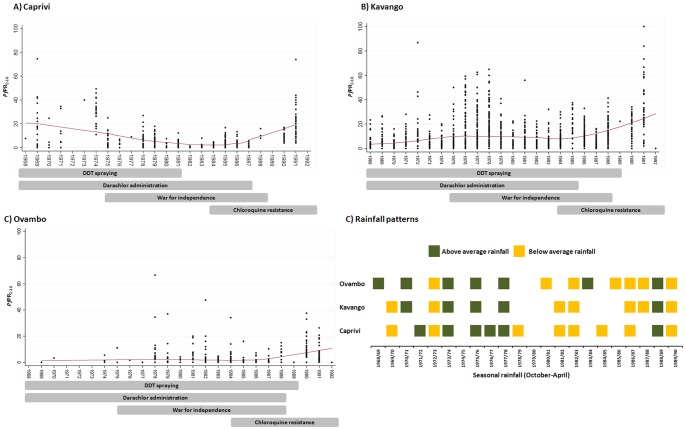
Methods: Community-based Plasmodium falciparum prevalence data from 3,260 geo-coded time-space locations between 1969 and 1992 were assembled from archives covering an examination of 230,174 individuals located in northern Namibia. These data were standardized the age-range 2 to less than 10 years and used within a Bayesian model-based geo-statistical framework to examine the changes of malaria risk in the years 1969, 1974, 1979, 1984 and 1989 at 5×5 km spatial resolution. This changing risk was described against rainfall seasons and the wide-scale use of indoor-residual house-spraying and mass drug administration.
Results: Most areas of Northern Namibia experienced low intensity transmission during a ten-year period of wide-scale control activities between 1969 and 1979. As control efforts waned, flooding occurred, drug resistance emerged and the war for independence intensified the spatial extent of moderate-to-high malaria transmission expanded reaching a peak in the late 1980s.
Conclusions: Targeting vectors and parasite in northern Namibia was likely to have successfully sustained a situation of low intensity transmission, but unraveled quickly to a peak of transmission intensity following a sequence of events by the early 1990s.
Conflict of interest statement
Figures
References
-
- The Malaria Elimination 8 Group website. Available: http://www.sadc.int/english/regional-integration/shdsp/sarn/elimination-.... Accessed Apr 10 2012.
-
- Ministry of Health and Social Services (2010). National Vector Borne Diseases Control Programme. Ministry of Health and Social Services. National Malaria Strategic Plan.
-
- Snow RW, Alegana VA, Makomva K, Reich A, Uusiku P, et al... (2010). Estimating the distribution of malaria in Namibia in 2009: assembling the evidence and modeling risk. Ministry of Health & Social Services, Republic of Namibia & Malaria Atlas Project.
-
- Hansford CF (1990). Malaria Control in Namibia. National Institute for Tropical Disease. Tzaneen, South Africa: Department of National Health and Population Development, (unpublished document).
-
- Kamwi RN (2005). Malaria Situation in Namibia. A Study of Vector Species and Effectiveness of the Past and Current Control Strategies in Selected Parts of Namibia [PhD thesis].Namibia: University of Namibia.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
