

The second face of blindness: processing speed deficits in the intact visual field after pre- and post-chiasmatic lesions
- PMID: 23667657
- PMCID: PMC3648511
- DOI: 10.1371/journal.pone.0063700
The second face of blindness: processing speed deficits in the intact visual field after pre- and post-chiasmatic lesions
Abstract
Purpose: Damage along the visual pathway results in a visual field defect (scotoma), which retinotopically corresponds to the damaged neural tissue. Other parts of the visual field, processed by the uninjured tissue, are considered to be intact. However, perceptual deficits have been observed in the "intact" visual field, but these functional impairments are poorly understood. We now studied temporal processing deficits in the intact visual field of patients with either pre- or post-chiasmatic lesions to better understand the functional consequences of partial blindness.
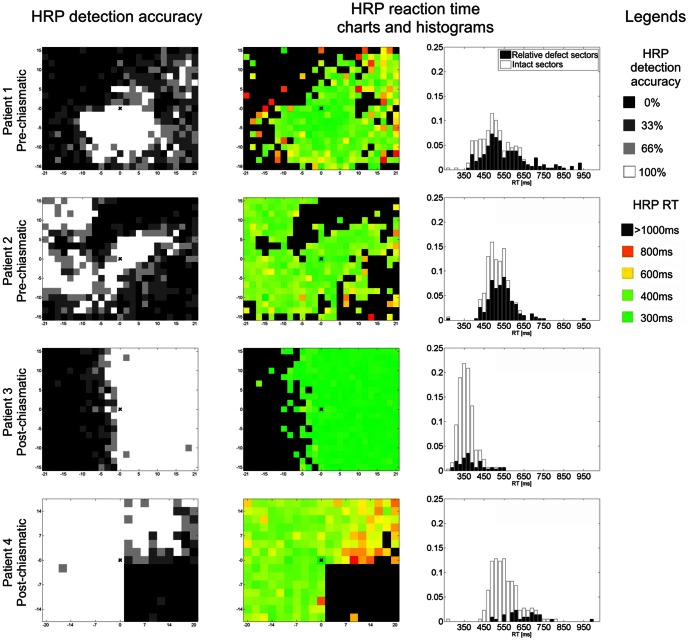
Methods: Patients with pre- (n = 53) or post-chiasmatic lesions (n = 98) were tested with high resolution perimetry--a method used to map visual fields with supra-threshold light stimuli. Reaction time of detections in the intact visual field was then analyzed as an indicator of processing speed and correlated with features of the visual field defect.
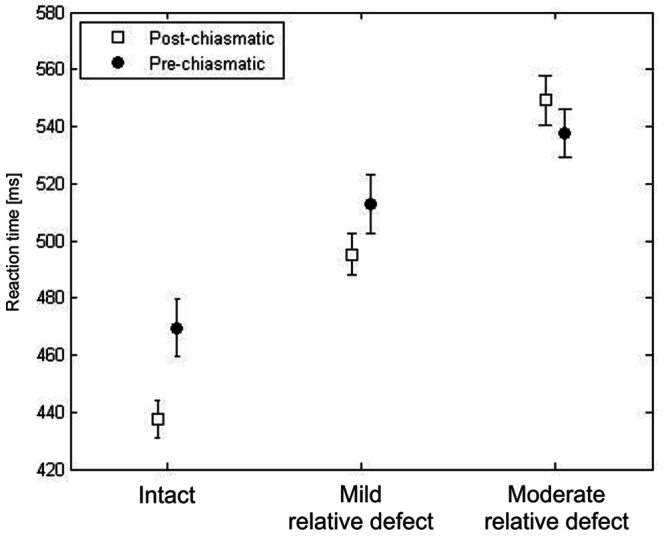
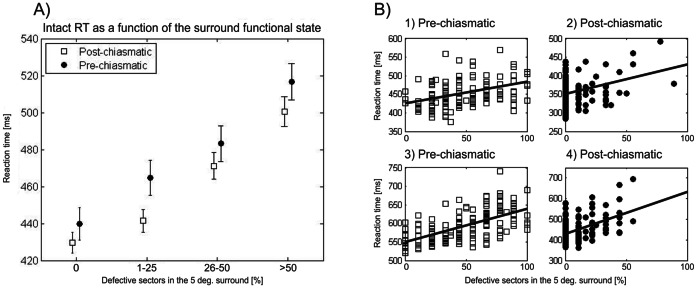
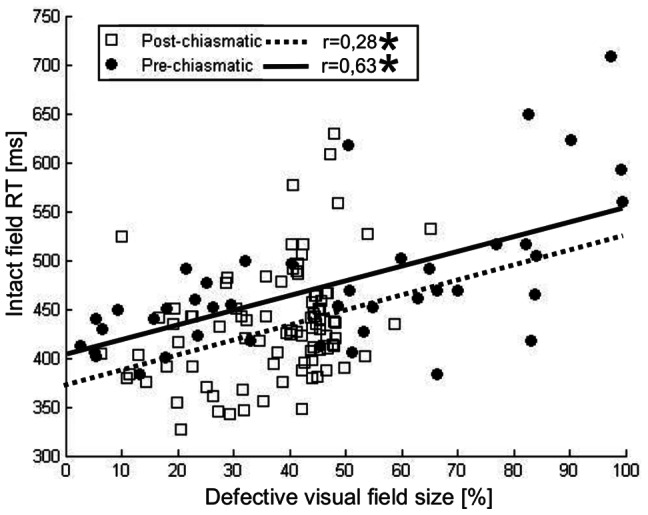
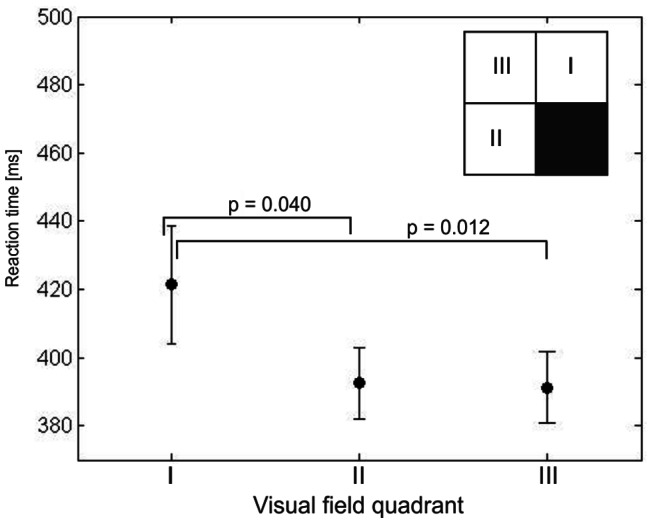
Results: Patients from both groups exhibited processing speed deficits in their presumably "intact" field as indicated by comparison to a normative sample. Further, in both groups processing speed was found to be a function of two factors. Firstly, a spatially restricted (retinotopic) influence of the scotoma was seen in longer reaction times when stimuli were presented in intact field sectors close to the defect. Secondly, patients with larger scotomata had on average longer reaction times in their intact field indicating a more general (non-retinotopic) influence of the scotoma.
Conclusions: Processing speed deficits in the "intact" visual field of patients with visual system damage demonstrate that visual system lesions have more widespread consequences on perception than previously thought. Because dysfunctions of the seeing field are expected to contribute to subjective vision, including visual tests of the presumed "intact" field may help to better understand vision loss and to improve methods of vision restoration and rehabilitation.
Conflict of interest statement
Figures
References
-
- Kollias SS, Landau K, Khan N, Golay X, Bernays R, et al. (1998) Functional evaluation using magnetic resonance imaging of the visual cortex in patients with retrochiasmatic lesions. J Neurosurg 89: 780–790. - PubMed
-
- Plow EB, Maguire S, Obretenova S, Pascual-Leone A, Merabet LB (2009) Approaches to rehabilitation for visual field defects following brain lesions. Expert Rev Med Devices 6: 291–305. - PubMed
-
- Sabel BA, Fedorov A, Henrich-Noack P, Gall C (2011) Vision restoration after brain damage: The “Residual Vision Activation Theory”. Prog Brain Res 192: 199–262. - PubMed
-
- Pöppel E, Held R, Frost D (1973) Residual visual function after brain wounds involving the central visual pathways in man. Nature 243: 295–296. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
