

Stereotactic body radiotherapy for localized prostate cancer: disease control and quality of life at 6 years
- PMID: 23668632
- PMCID: PMC3674983
- DOI: 10.1186/1748-717X-8-118
Stereotactic body radiotherapy for localized prostate cancer: disease control and quality of life at 6 years
Abstract
Background: Stereotactic body radiotherapy (SBRT) may yield disease control for prostate cancer in a brief, hypofractionated treatment regimen without increasing treatment toxicity. Our report presents a 6-year update from 304 low- (n = 211), intermediate- (n = 81), and high-risk (n = 12) prostate cancer patients who received CyberKnife SBRT.
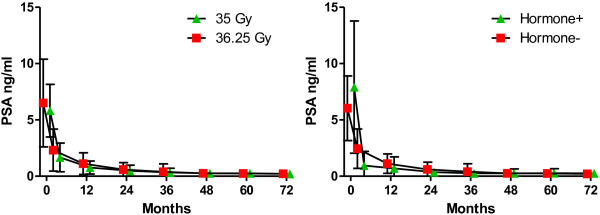
Methods: The median PSA at presentation was 5.8 ng/ml. Fifty-seven patients received neoadjuvant hormonal therapy for up to one year. The first 50 patients received a total dose of 35 Gy in 5 fractions of 7 Gy. The subsequent 254 patients received a total dose of 36.25 Gy in 5 fractions of 7.25 Gy. Toxicity was assessed with the Expanded Prostate Cancer Index Composite questionnaire and the Radiation Therapy Oncology Group urinary and rectal toxicity scale. Biochemical failure was assessed using the nadir + 2 definition.
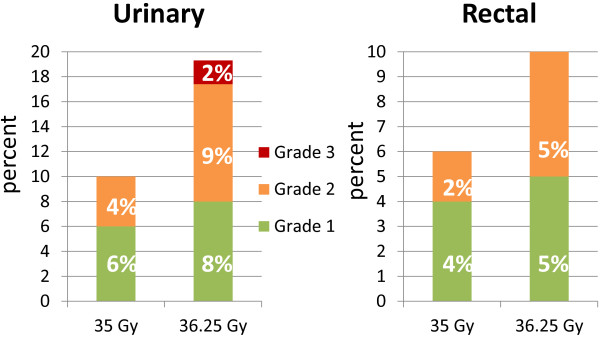
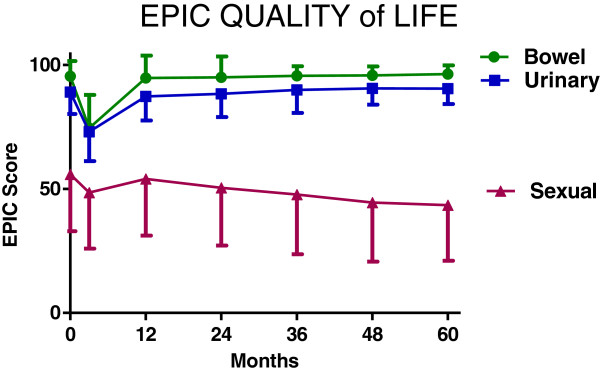
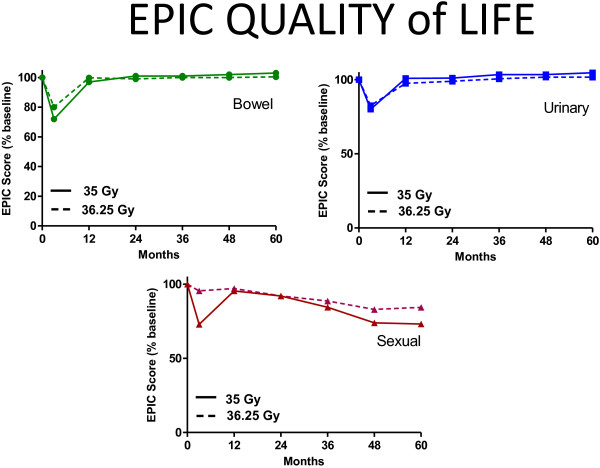
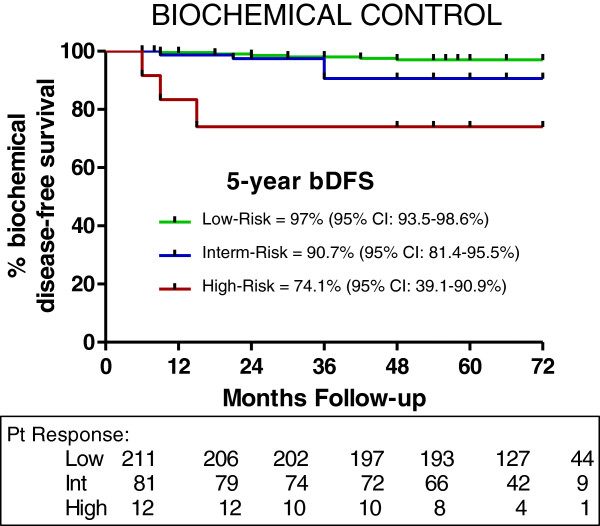
Results: No patients experienced Grade III or IV acute complications. Fewer than 5% of patients experienced any acute Grade II urinary or rectal toxicities. Late urinary Grade II complications were observed in 4% of patients treated to 35 Gy and 9% of patients treated to 36.25 Gy. Five (2%) late Grade III urinary toxicities occurred in patients who were treated with 36.25 Gy. Late Grade II rectal complications were observed in 2% of patients treated to 35 Gy and 5% of patients treated to 36.25 Gy. Bowel and urinary quality of life (QOL) scores initially decreased, but later returned to baseline values. An overall decrease of 20% in the sexual QOL score was observed. QOL in each domain was not differentially affected by dose. For patients that were potent prior to treatment, 75% stated that they remained sexually potent. Actuarial 5-year biochemical recurrence-free survival was 97% for low-risk, 90.7% for intermediate-risk, and 74.1% for high-risk patients. PSA fell to a median of 0.12 ng/ml at 5 years; dose did not influence median PSA levels.
Conclusions: In this large series with long-term follow-up, we found excellent biochemical control rates and low and acceptable toxicity, outcomes consistent with those reported for from high dose rate brachytherapy (HDR BT). Provided that measures are taken to account for prostate motion, SBRT's distinct advantages over HDR BT include its noninvasiveness and delivery to patients without anesthesia or hospitalization.
Figures
References
-
- Potosky AL, Legler J, Albertsen PC, Stanford JL, Gilliland FD, Hamilton AS, Eley JW, Stephenson RA, Harlan LC. Health outcomes after prostatectomy or radiotherapy for prostate cancer: results from the prostate cancer outcomes study. J Natl Cancer Inst. 2000;92:1582–1592. doi: 10.1093/jnci/92.19.1582. - DOI - PubMed
-
- Force USPST. Screening for prostate cancer: U.S. Preventive services task force recommendation statement. Ann Intern Med. 2008;149:185–191. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
