

Subcellular mislocalization of the transcription factor NF-E2 in erythroid cells discriminates prefibrotic primary myelofibrosis from essential thrombocythemia
- PMID: 23670178
- PMCID: PMC3701907
- DOI: 10.1182/blood-2012-11-463257
Subcellular mislocalization of the transcription factor NF-E2 in erythroid cells discriminates prefibrotic primary myelofibrosis from essential thrombocythemia
Abstract
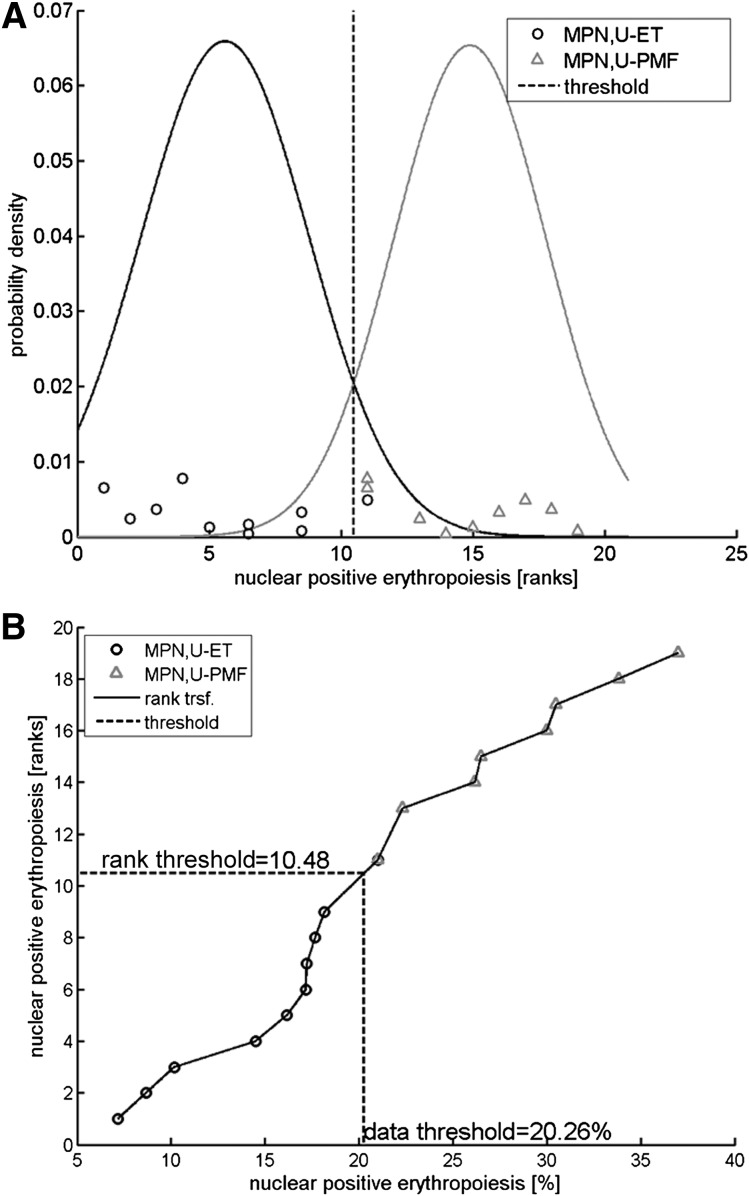
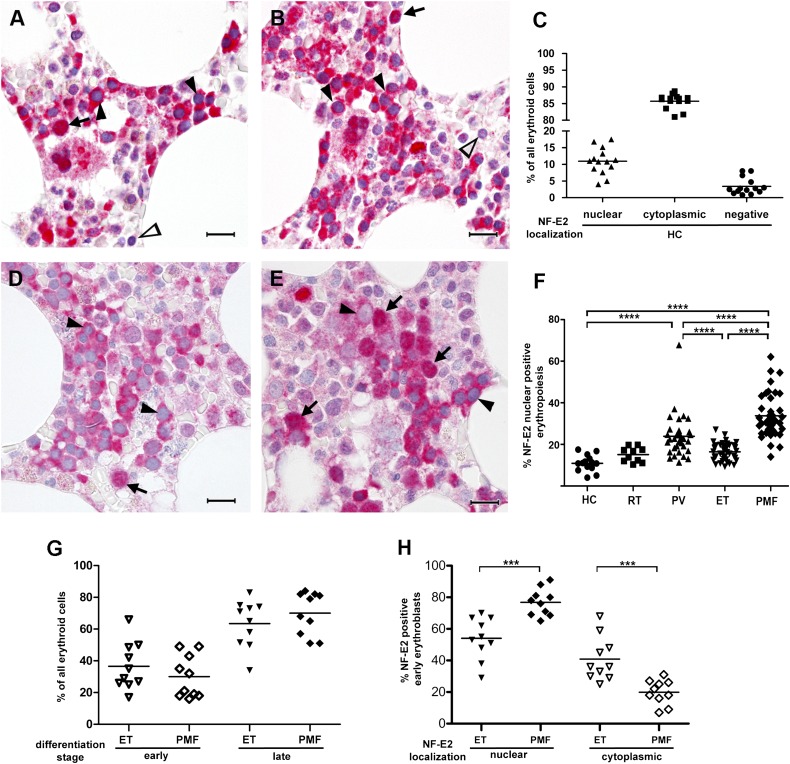
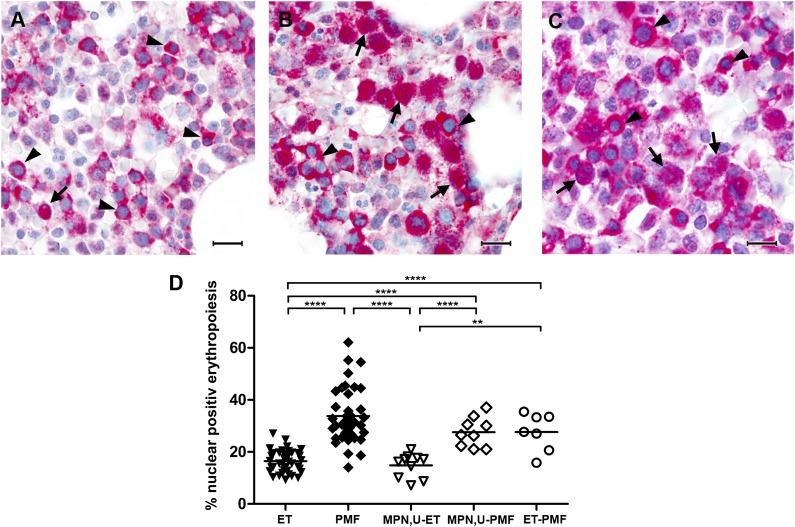
The World Health Organization (WHO) classification of myeloproliferative neoplasms (MPNs) comprises several entities including essential thrombocythemia (ET); primary myelofibrosis (PMF); and MPN, unclassifiable (MPN,U). Differential diagnosis between ET and early, prefibrotic PMF can be challenging but is critical because clinical course and outcome vary considerably between these entities. We have previously shown that the transcription factor nuclear factor erythroid 2 (NF-E2) is aberrantly expressed in MPN patients. Here we demonstrate that NF-E2 is mislocalized in PMF cells and that aberrant NF-E2 localization discriminates statistically highly significantly between ET and PMF. A threshold of 20% nuclear NF-E2 staining was cross-validated by ".682+ bootstrapping." Moreover, this cutoff correctly classifies diagnostic bone marrow biopsies of MPN,U patients specified upon follow-up as ET or PMF with 92% accuracy. Because interobserver concordance between independent pathologists was high (Spearman's rank correlation coefficient, 0.727), we propose that quantitative NF-E2 immunohistochemistry represents a diagnostic tool that can reliably support a differential diagnosis between ET and PMF.
Figures
References
-
- Dameshek W. Some speculations on the myeloproliferative syndromes. Blood. 1951;6(4):372–375. - PubMed
-
- Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissue. In: Bosman FT, Jaffe ES, Lakhani SR, et al., editors. WHO Classification of Tumours, vol. 4. Lyon, France: IARC Press; 2008.
-
- James C, Ugo V, Le Couédic JP, et al. A unique clonal JAK2 mutation leading to constitutive signalling causes polycythaemia vera. Nature. 2005;434(7037):1144–1148. - PubMed
-
- Baxter EJ, Scott LM, Campbell PJ, et al. Cancer Genome Project. Acquired mutation of the tyrosine kinase JAK2 in human myeloproliferative disorders. Lancet. 2005;365(9464):1054–1061. - PubMed
-
- Kralovics R, Buser AS, Teo SS, et al. Comparison of molecular markers in a cohort of patients with chronic myeloproliferative disorders. Blood. 2003;102(5):1869–1871. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
