

A prospective randomized study comparing isolation of the arrhythmogenic vein versus all veins in paroxysmal atrial fibrillation
- PMID: 23670880
- PMCID: PMC6649468
- DOI: 10.1002/clc.22132
A prospective randomized study comparing isolation of the arrhythmogenic vein versus all veins in paroxysmal atrial fibrillation
Abstract
Background: Ablation procedures in patients with paroxysmal atrial fibrillation (PAF) includes isolation of all pulmonary veins (PVs). We hypothesized that an approach using an algorithm to detect arrhythmogenic PVs (aPVs) might lead to shorter procedure duration (PD) and fewer proarrhythmic effects (PE).
Hypothesis: Isolation of the aPVs only leads to a reduced PD, reduced PEs, and fewer adverse events, with a success rate comparable to the standard all-PV approach.
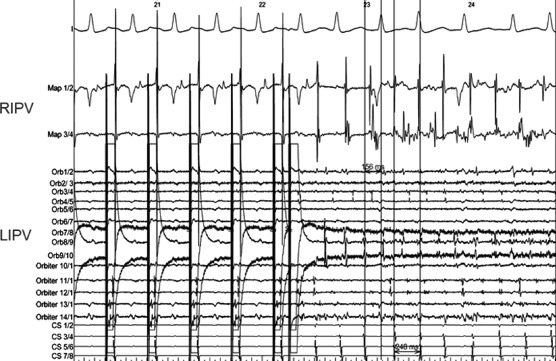
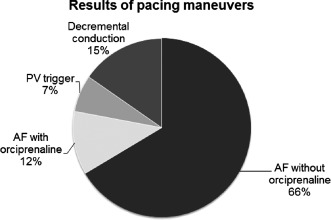
Methods: In this prospective trial, 207 patients with PAF were randomized to undergo isolation of the aPV (AG group, n = 105) or isolation of all PVs (VG group, n = 102). The aPV was identified by atrial fibrillation (AF) induction, focal discharge, or short local PV decremental conduction during PV pacing. Patients were followed with repetitive 7-day Holter electrocardiograms (ECGs) after 3, 6, and 12 months in our arrhythmia clinic.
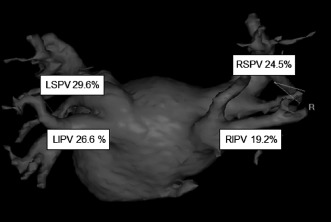
Results: In 97% of patients, at least 1 aPV was identified (mean, 2.1). PD did not differ significantly (152.3 ± 57.1 minutes vs 162 ± 68 minutes, P = 0.27) between the groups, but the number of radiofrequency (RF) applications and fluoroscopy time (FT) and dose were significantly lower in the AG group than in the VG group. The occurrence of PE (new-onset atrial tachycardia) and adverse events (AE) did not differ between the 2 groups (P = 0.1). Sinus rhythm off antiarrhythmic medication (documented on 7-day Holter ECGs) 12 months after a single procedure was achieved in 53% in the AG group and 59% in the VG group (P = 0.51).
Conclusions: Isolation of the aPVs detected by a straightforward algorithm leads to similar success rates compared to a standard all-PV approach with regard to PD, AE, or PE and is associated with less RF and a shorter FT.
Trial registration: ClinicalTrials.gov NCT00605748.
© 2013 Wiley Periodicals, Inc.
Figures
Similar articles
-
Efficacy of selective arrhythmogenic pulmonary veins isolation versus empirical all pulmonary veins isolation for atrial fibrillation: a meta-analysis of randomized and observational studies.J Interv Card Electrophysiol. 2014 Apr;39(3):233-40. doi: 10.1007/s10840-013-9865-8. Epub 2014 Feb 20. J Interv Card Electrophysiol. 2014. PMID: 24554249 Review.
-
Functional disconnection of arrhythmogenic pulmonary veins in patients with paroxysmal atrial fibrillation guided by combined electroanatomical (CARTO) and conventional mapping.J Interv Card Electrophysiol. 2002 Jul;6(3):267-75. doi: 10.1023/a:1019565921739. J Interv Card Electrophysiol. 2002. PMID: 12154329
-
Influence of energy source on early atrial fibrillation recurrences: a comparison of cryoballoon vs. radiofrequency current energy ablation with the endpoint of unexcitability in pulmonary vein isolation.Europace. 2018 Jan 1;20(1):43-49. doi: 10.1093/europace/euw307. Europace. 2018. PMID: 27742775 Clinical Trial.
-
Randomized Study of Persistent Atrial Fibrillation Ablation: Ablate in Sinus Rhythm Versus Ablate Complex-Fractionated Atrial Electrograms in Atrial Fibrillation.Circ Arrhythm Electrophysiol. 2016 Feb;9(2):e003596. doi: 10.1161/CIRCEP.115.003596. Circ Arrhythm Electrophysiol. 2016. PMID: 26857909 Clinical Trial.
-
Cryoballoon versus radiofrequency for pulmonary vein re-isolation after a failed initial ablation procedure in patients with paroxysmal atrial fibrillation.J Cardiovasc Electrophysiol. 2013 Mar;24(3):274-9. doi: 10.1111/jce.12038. Epub 2012 Dec 4. J Cardiovasc Electrophysiol. 2013. PMID: 23210695 Clinical Trial.
Cited by
-
Comparing Efficacy and Safety in Catheter Ablation Strategies for Paroxysmal Atrial Fibrillation: A Network Meta-Analysis of Randomized Controlled Trials.Diagnostics (Basel). 2022 Feb 9;12(2):433. doi: 10.3390/diagnostics12020433. Diagnostics (Basel). 2022. PMID: 35204535 Free PMC article. Review.
-
Efficacy of selective arrhythmogenic pulmonary veins isolation versus empirical all pulmonary veins isolation for atrial fibrillation: a meta-analysis of randomized and observational studies.J Interv Card Electrophysiol. 2014 Apr;39(3):233-40. doi: 10.1007/s10840-013-9865-8. Epub 2014 Feb 20. J Interv Card Electrophysiol. 2014. PMID: 24554249 Review.
-
Comparing efficacy and safety in catheter ablation strategies for atrial fibrillation: a network meta-analysis.BMC Med. 2022 May 31;20(1):193. doi: 10.1186/s12916-022-02385-2. BMC Med. 2022. PMID: 35637488 Free PMC article.
-
Selective Versus Total Pulmonary Vein Isolation In Atrial Fibrillation Ablation.J Atr Fibrillation. 2014 Jun 30;7(1):999. doi: 10.4022/jafib.999. eCollection 2014 Jun-Jul. J Atr Fibrillation. 2014. PMID: 27957072 Free PMC article. Review.
References
-
- Haissaguerre M, Jais P, Shah DC, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998;339:659–666. - PubMed
-
- Jais P, Hocini M, Macle L, et al. Distinctive electrophysiological properties of pulmonary veins in patients with atrial fibrillation. Circulation. 2002;106:2479–2485. - PubMed
-
- Deisenhofer I, Estner H, Reents T, et al. Does electrogram guided substrate ablation add to the success of pulmonary vein isolation in patients with paroxysmal atrial fibrillation? A prospective, randomized study. J Cardiovasc Electrophysiol. 2009;20:514–521. - PubMed
-
- Karch MR, Zrenner B, Deisenhofer I, et al. Freedom from atrial tachyarrhythmias after catheter ablation of atrial fibrillation: a randomized comparison between 2 current ablation strategies. Circulation. 2005;111:2875–2880. - PubMed
-
- Gerstenfeld EP, Sauer W, Callans DJ, et al. Predictors of success after selective pulmonary vein isolation of arrhythmogenic pulmonary veins for treatment of atrial fibrillation. Heart Rhythm. 2006;3:165–170. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
