

Biochemistry of adipose tissue: an endocrine organ
- PMID: 23671428
- PMCID: PMC3648822
- DOI: 10.5114/aoms.2013.33181
Biochemistry of adipose tissue: an endocrine organ
Abstract
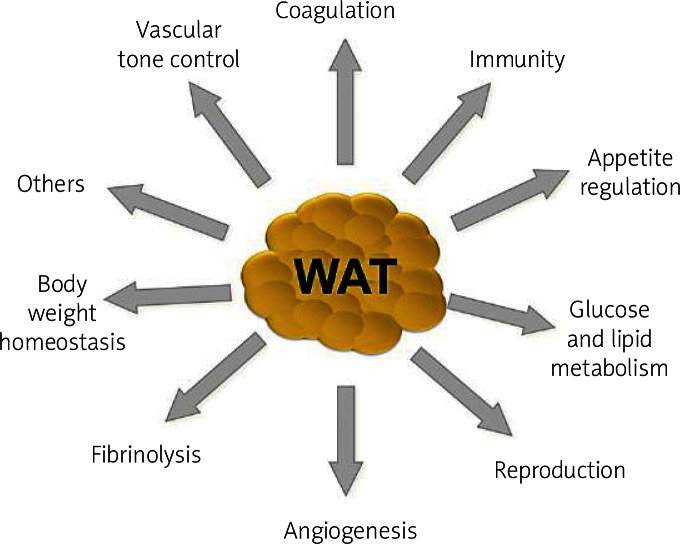
Adipose tissue is no longer considered to be an inert tissue that stores fat. This tissue is capable of expanding to accommodate increased lipids through hypertrophy of existing adipocytes and by initiating differentiation of pre-adipocytes. Adipose tissue metabolism exerts an impact on whole-body metabolism. As an endocrine organ, adipose tissue is responsible for the synthesis and secretion of several hormones. These are active in a range of processes, such as control of nutritional intake (leptin, angiotensin), control of sensitivity to insulin and inflammatory process mediators (tumor necrosis factor α (TNF-α), interleukin-6 (IL-6), resistin, visfatin, adiponectin, among others) and pathways (plasminogen activator inhibitor 1 (PAI-1) and acylation stimulating protein (ASP) for example). This paper reviews some of the biochemical and metabolic aspects of adipose tissue and its relationship to inflammatory disease and insulin resistance.
Keywords: adipocytes; adipokines; adipose tissue.
Figures



References
-
- Ottaviani E, Malagoli D, Franceschi C. The evolution of the adipose tissue: a neglected enigma. Gen Comp Endocrinol. 2011;174:1–4. - PubMed
-
- Bernlohr DA, Jenkins AE, Bennaars AA. Adipose tissue and lipid metabolism. In: Vence JE, Vence D, editors. Biochemistry of lipids, lipoproteins and membranes. 4th ed. Elsevier Science: Amsterdam; 2002. pp. 263–89.
-
- Ahima RS, Flier JS. Adipose tissue as an endocrine organ. Trends Endocrinol Metab. 2000;11:327–32. - PubMed
-
- Fonseca-Alaniz MH, Takada J, Alonso-Vale MIC, Lima FB. Adipose tissue as an endocrine organ: from theory to practice. J Pediatr. 2007;83:S192–203. - PubMed
-
- Saely C, Geiger K, Drexel H. Browns versus white adipose tissue: a mini-review. Gerontol. 2012;58:120–2. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous