

From multidrug- to extensively drug-resistant tuberculosis: upward trends as seen from a 15-year nationwide study
- PMID: 23671662
- PMCID: PMC3650045
- DOI: 10.1371/journal.pone.0063128
From multidrug- to extensively drug-resistant tuberculosis: upward trends as seen from a 15-year nationwide study
Abstract
Background: Emergence of extensively drug-resistant tuberculosis (XDR-TB) represents an enormous challenge to Public Health globally.
Methods: Progression towards XDR-TB was investigated in Belgium, a country with a typically low TB incidence, by analyzing the magnitude, characteristics, and treatment success of multidrug-resistant tuberculosis (MDR-TB) through a population-based study from 1994 to 2008.
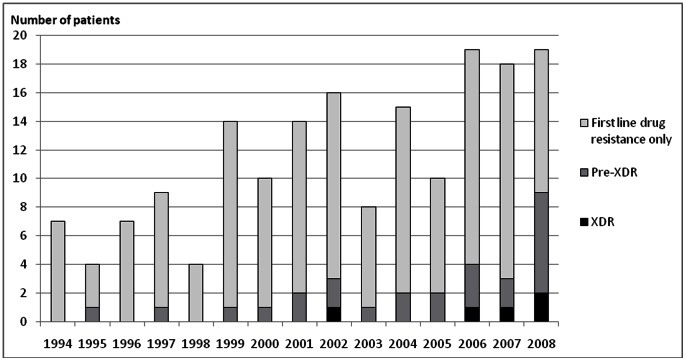
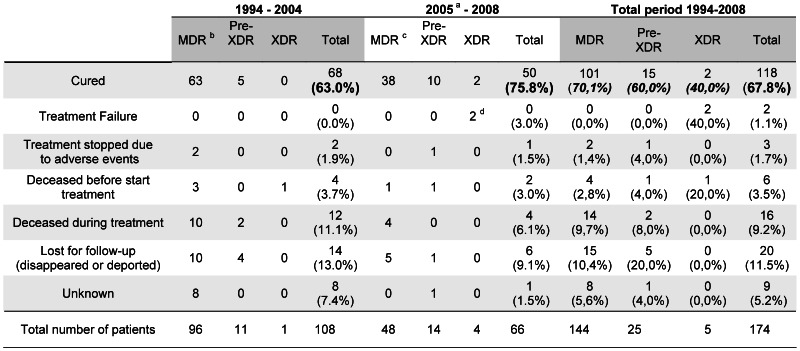
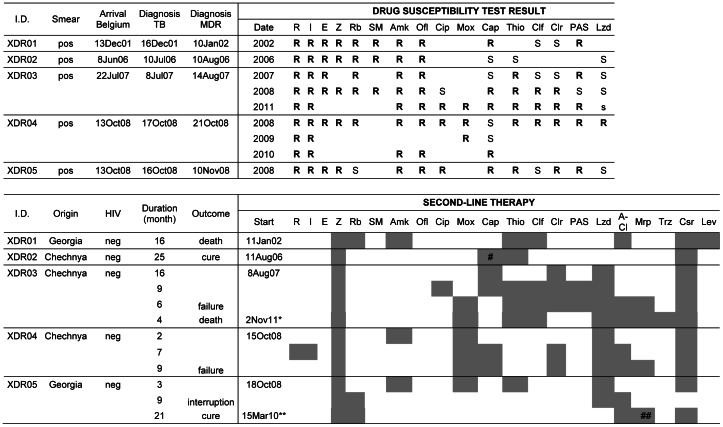
Results: Among the 174 MDR-TB patients, 81% were foreign-born, 48% of these being asylum seekers. Although the number of MDR-TB patients remained stable through the study period at around 15 new cases annually, frequencies of resistance of the patients' first MDR-TB isolate to second-line drugs increased, as well as the total number of antibiotics it was resistant to (p<0.001). XDR-TB cases were detected from 2002 onwards. For 24 patients, additional resistance to several second-line drugs was acquired during treatment. Molecular-guided investigations indicated little to no contribution of in-country clonal spread or exogenous re-infection. The increase of pre-XDR and XDR cases could be attributed to rising proportions of patients from Asia and Central and Eastern Europe (p<0.001) and an increase in the isolation of Beijing strains in these groups (p<0.001). Despite augmented resistance, the treatment success rate improved from 63.0% to 75.8% (p = 0.080) after implementation in 2005 of improved surveillance measures and therapeutic access.
Conclusions: Increasing severity in drug resistance patterns leading to more XDR- and "panresistant" TB cases in a country with a low TB incidence like Belgium represents a strong alert on worsening situations in other world regions and requires intense public health measures.
Conflict of interest statement
Figures
References
-
- Van Rie A, Enarson D (2006) XDR tuberculosis: an indicator of public-health negligence. Lancet 368: 1554–1556. - PubMed
-
- MMWR (2006) Emergence of Mycobacterium tuberculosis with extensive resistance to second-line drugs-worldwide, 2000–2004. MMWR Morb Mortal Wkly Rep 55: 301–305. - PubMed
-
- Migliori GB, Loddenkemper R, Blasi F, Raviglione MC (2007) 125 years after Robert Koch's discovery of the tubercle bacillus: the new XDR-TB threat. Is “science” enough to tackle the epidemic? Eur Respir J 29: 423–427. - PubMed
-
- Velayati AA, Masjedi MR, Farnia P, Tabarsi P, Ghanavi J, et al. (2009) Emergence of new forms of totally drug-resistant tuberculosis bacilli: super extensively drug-resistant tuberculosis or totally drug-resistant strains in iran. Chest 136: 420–425. - PubMed
-
- Udwadia ZF, Amale RA, Ajbani KK, Rodrigues C (2012) Totally drug-resistant tuberculosis in India. Clin Infect Dis 54: 579–581. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
