

Endovascular treatment of carotid cavernous sinus fistula: A systematic review
- PMID: 23671750
- PMCID: PMC3647206
- DOI: 10.4329/wjr.v5.i4.143
Endovascular treatment of carotid cavernous sinus fistula: A systematic review
Abstract
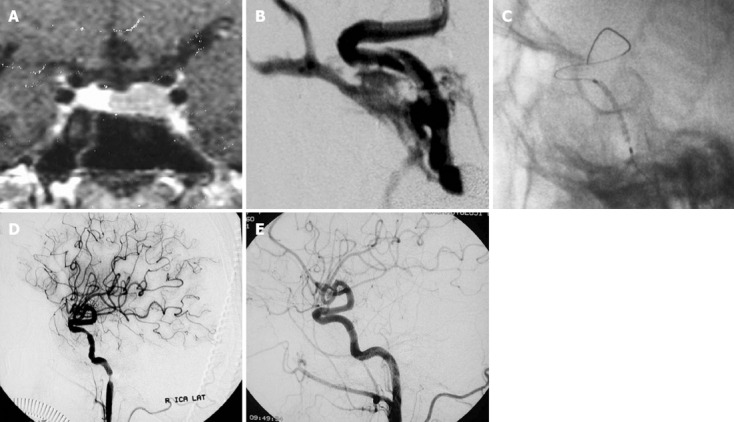
Carotid cavernous sinus fistulas are abnormal communications between the carotid system and the cavernous sinus. Several classification schemes have described carotid cavernous sinus fistulas according to etiology, hemodynamic features, or the angiographic arterial architecture. Increased pressure within the cavernous sinus appears to be the main factor in pathophysiology. The clinical features are related to size, exact location, and duration of the fistula, adequacy and route of venous drainage and the presence of arterial/venous collaterals. Noninvasive imaging (computed tomography, magnetic resonance, computed tomography angiography, magnetic resonance angiography, Doppler) is often used in the initial work-up of a possible carotid cavernous sinus fistulas. Cerebral angiography is the gold standard for the definitive diagnosis, classification, and planning of treatment for these lesions. The endovascular approach has evolved as the mainstay therapy for definitive treatment in situations including clinical emergencies. Conservative treatment, surgery and radiosurgery constitute other management options for these lesions.
Keywords: Carotid cavernous sinus fistula; Cavernous sinus; Endovascular treatment.
Figures




References
-
- Barrow DL, Spector RH, Braun IF, Landman JA, Tindall SC, Tindall GT. Classification and treatment of spontaneous carotid-cavernous sinus fistulas. J Neurosurg. 1985;62:248–256. - PubMed
-
- Ernst RJ, Tomsick TA. Classification and angiography of carotid cavernous fistulas. In: Tomsick TA, editor. Carotid cavernous sinus fistula. Cincinnati: Digital Education Publishing; 1997. pp. 13–22.
-
- Ringer AJ, Salud L, Tomsick TA. Carotid cavernous fistulas: anatomy, classification, and treatment. Neurosurg Clin N Am. 2005;16:279–295. - PubMed
-
- Tjoumakaris SI, Jabbour PM, Rosenwasser RH. Neuroendovascular management of carotid cavernous fistulae. Neurosurg Clin N Am. 2009;20:447–452. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
